Neuroscience and Ophthalmology, Institute of Inflammation and Ageing, College of Medical and Dental Sciences, University of Birmingham, Birmingham, UK; School of Biomedical Sciences, Institute of Clinical Sciences, College of Medical and Dental Sciences, University of Birmingham, Birmingham, UK.
Neuroscience and Ophthalmology, Institute of Inflammation and Ageing, College of Medical and Dental Sciences, University of Birmingham, Birmingham, UK; Ophthalmology Department, University Hospitals Birmingham NHS Foundation Trust, Birmingham, UK.
Exp Eye Res. 2020 Aug;197:108102. doi: 10.1016/j.exer.2020.108102. Epub 2020 Jun 6.
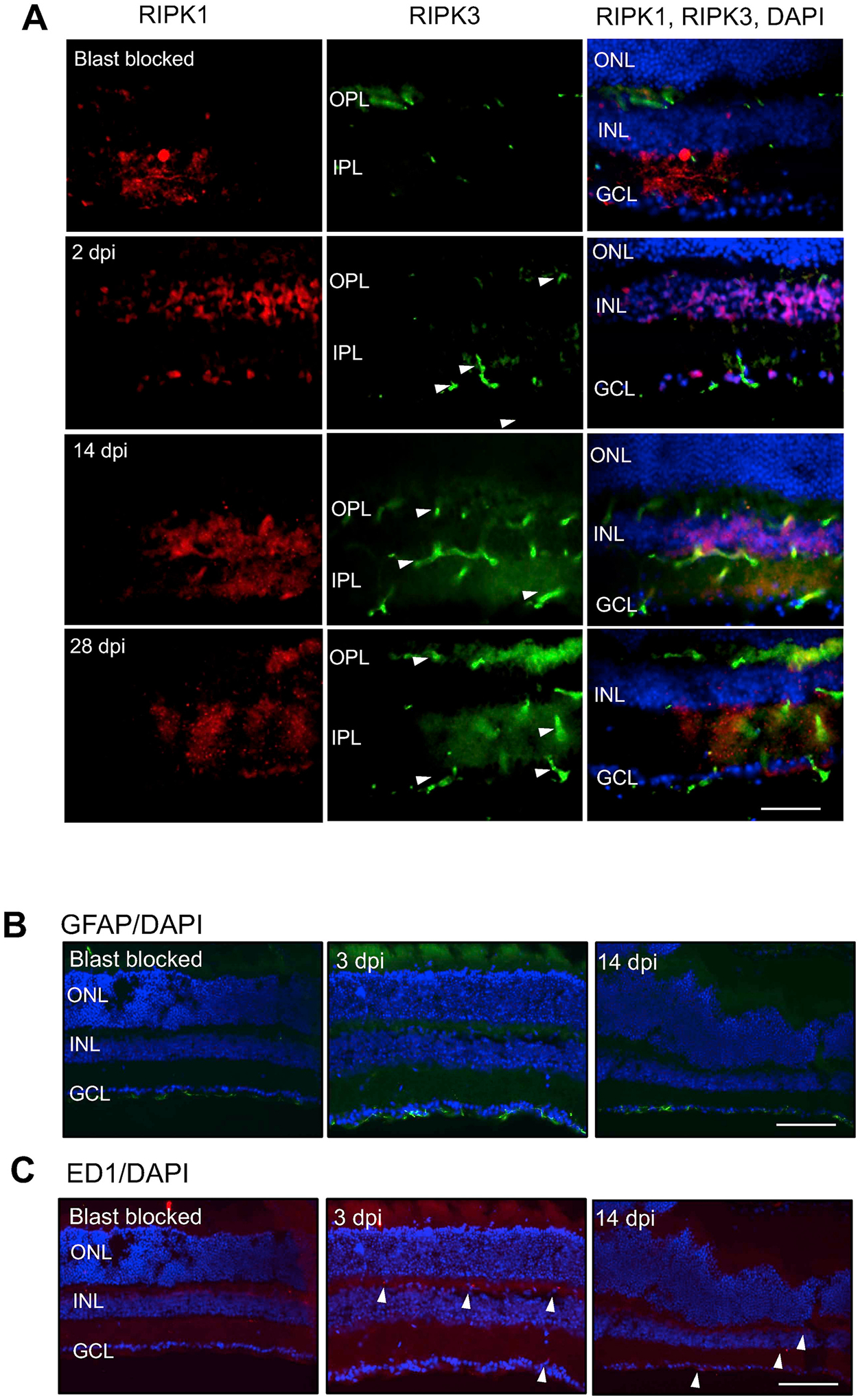
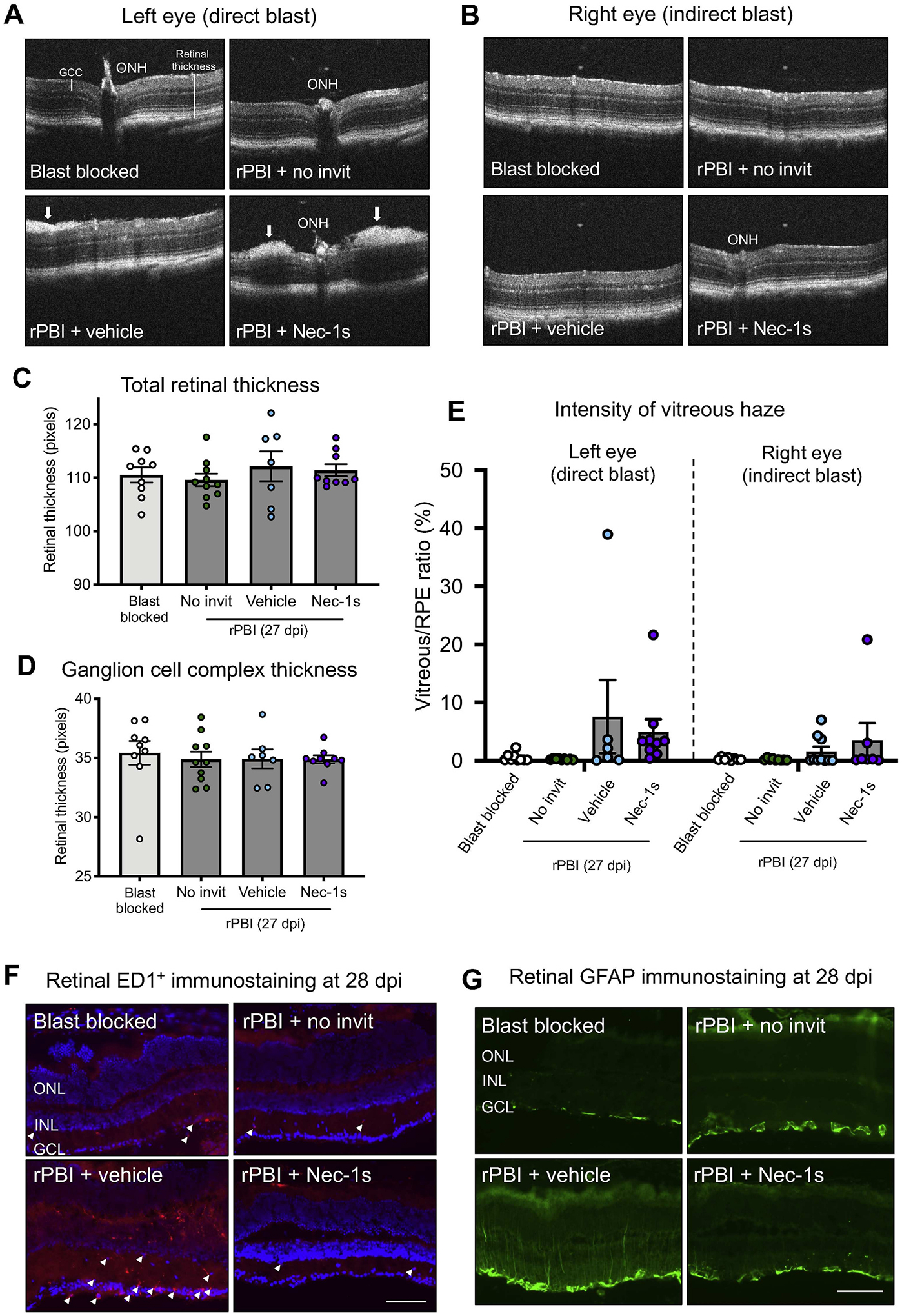
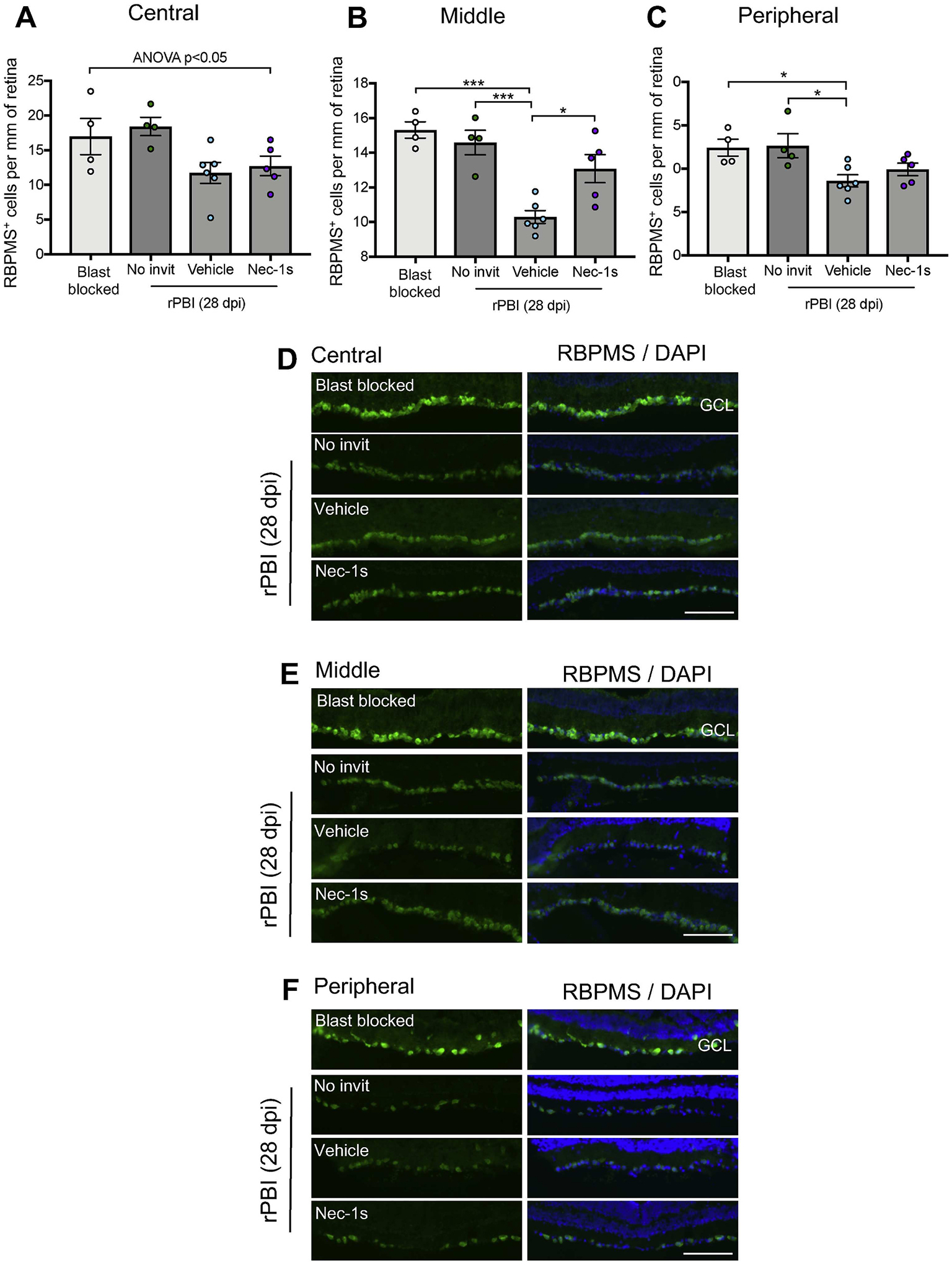
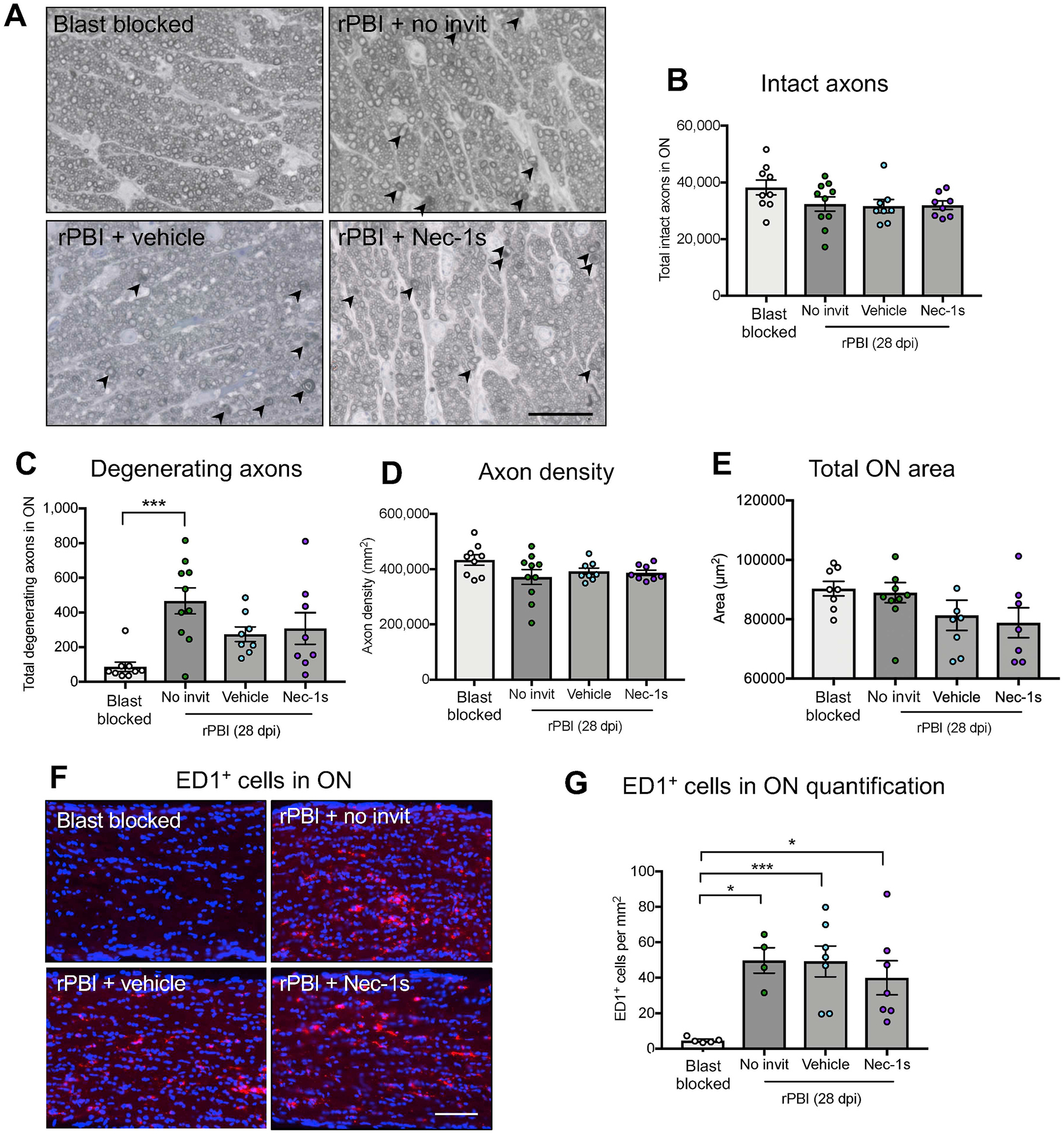
Primary blast injury (caused by the initial rapid increase in pressure following an explosive blast) to the retina and optic nerve (ON) causes progressive visual loss and neurodegeneration. Military personnel are exposed to multiple low-overpressure blast waves, which may be in quick succession, such as during breacher training or in combat. We investigated the necroptotic cell death pathway in the retina in a mouse repeated primary ocular blast injury (rPBI) model using immunohistochemistry. We further evaluated whether intravitreal injections of a potent necroptosis inhibitor, Necrostatin-1s (Nec-1s), protects the retina and ON axons by retinal ganglion cells (RGC) counts, ON axonal counting and optical coherence tomography (OCT) analysis of vitreous haze. Receptor interacting protein kinase (RIPK) 3, increased in the inner plexiform layer 2 days post injury (dpi) and persisted until 14 dpi, whilst RIPK1 protein expression did not change after injury. The number of degenerating ON axons was increased at 28 dpi but there was no evidence of a reduction in the number of intact ON axons or RNA-binding protein with multiple splicing (RBPMS) RGC in the retina by 28 dpi in animals not receiving any intravitreal injections. But, when intravitreal injections (vehicle or Nec-1s) were given there was a significant reduction in RBPMS RGC numbers, suggesting that rPBI with intraocular injections is damaging to RGC. There were fewer RGC lost after Nec-1s than vehicle injection, but there was no effect of Nec-1s or vehicle treatment on the number of degenerating axons. OCT analysis demonstrated no effect of rPBI on vitreous haze, but intravitreal injection combined with rPBI increased vitreous haze (P = 0.004). Whilst necroptosis may be an active cell death signalling pathway after rPBI, its inhibition did not prevent cell death, and intravitreal injections in combination with rPBI increased vitreous inflammation and reduced RBPMS RGC numbers, implying intravitreal injection is not an ideal method for drug delivery after rPBI.
原发性爆炸伤(由爆炸后压力的快速增加引起)会导致视网膜和视神经(ON)逐渐丧失视力和发生神经退行性病变。军事人员会多次暴露于低超压爆炸波中,这些爆炸波可能会连续发生,例如在爆破手训练或战斗中。我们使用免疫组织化学法研究了小鼠反复原发性眼部爆炸伤(rPBI)模型中视网膜的坏死性细胞死亡途径。我们进一步评估了玻璃体内注射强效坏死抑制剂 Necrostatin-1s(Nec-1s)是否通过视网膜神经节细胞(RGC)计数、视神经轴突计数和玻璃体混浊的光学相干断层扫描(OCT)分析来保护视网膜和视神经轴突。伤后 2 天(dpi)内层神经节细胞层中 RIPK3 增加,并持续到 14 dpi,而 RIPK1 蛋白表达在损伤后没有改变。28 dpi 时,变性视神经轴突的数量增加,但在未接受任何玻璃体内注射的动物中,28 dpi 时 ON 轴突完整的数量或 RNA 结合蛋白多聚体(RBPMS)RGC 数量没有减少的证据。但是,当进行玻璃体内注射(载体或 Nec-1s)时,RBPMS RGC 数量明显减少,表明眼内注射 rPBI 会对 RGC 造成损害。与载体注射相比,Nec-1s 后丢失的 RGC 更少,但 Nec-1s 或载体处理对变性轴突的数量没有影响。OCT 分析表明 rPBI 对玻璃体混浊没有影响,但玻璃体内注射结合 rPBI 增加了玻璃体混浊(P=0.004)。虽然坏死性细胞死亡可能是 rPBI 后的一种活跃的细胞死亡信号通路,但它的抑制并不能阻止细胞死亡,并且玻璃体内注射结合 rPBI 增加了玻璃体炎症并减少了 RBPMS RGC 数量,这意味着玻璃体内注射不是 rPBI 后药物输送的理想方法。