Vitiello Paola, Sica Antonello, Ronchi Andrea, Caccavale Stefano, Franco Renato, Argenziano Giuseppe
Dermatology Unit, University of Campania Luigi Vanvitelli, Naples, Italy.
Department of Precision Medicine, University of Campania Luigi Vanvitelli, Naples, Italy.
Front Oncol. 2020 May 27;10:651. doi: 10.3389/fonc.2020.00651. eCollection 2020.
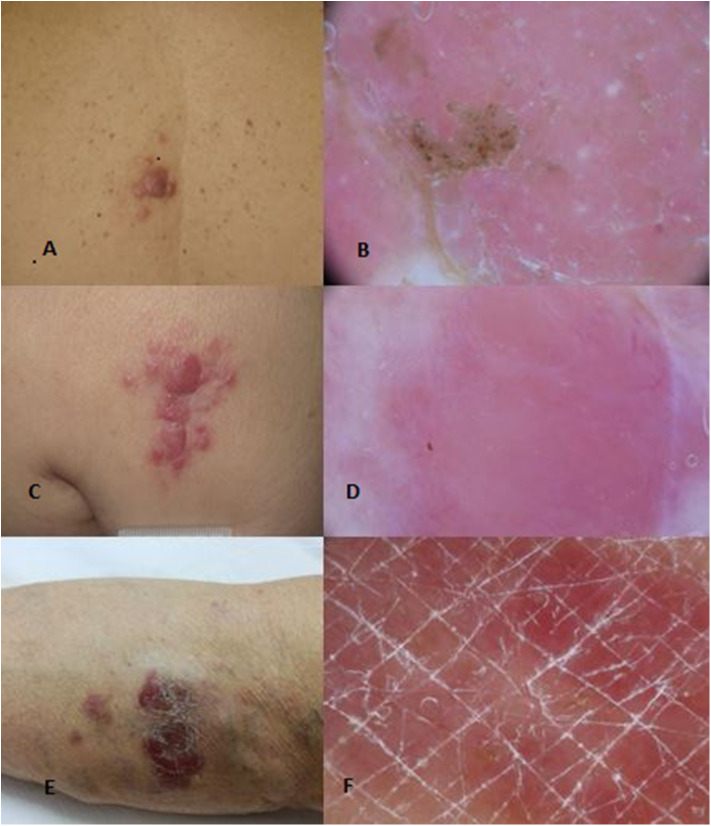
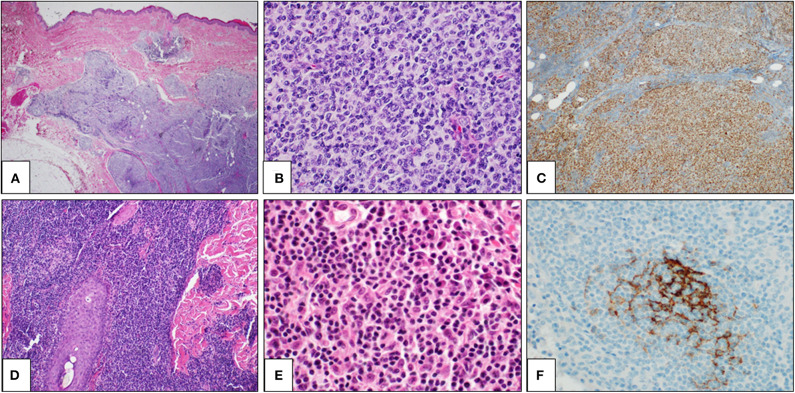
Primary cutaneous B-cell lymphomas (PCBCLs) comprise a group of extranodal B-cell non-Hodgkin lymphomas B-cell derived, which primarily involve the skin without evidence of extracutaneous disease at the time of diagnosis. They include ~25% of all cutaneous lymphomas and are classified in three major subgroups (World Health Organization (WHO) 2017): primary cutaneous marginal zone lymphoma (PCMZL), primary cutaneous follicle-center cell lymphoma (PCFCL), and diffuse large B-cell lymphoma, leg type (PCDLBCL, LT). This classification also includes some less common entities such as intravascular large B-cell lymphoma. Recently, WHO-EORTC added Epstein-Barr virus positive (EBV+) mucocutaneous ulcer, as a new provisional distinct entity, to cutaneous B-cell lymphomas. PCBCLs are classically characterized by patches, plaques, or nodules showing great variability for color, shape, and location. Diagnosis requires histological examination with immunohistochemical staining. In general, therapeutic options depend on the exact histological and immunohistochemical classification, disease presentation, and risk assessment. PCMZL and PCFCL are considered indolent lymphomas with a good prognosis and are associated with 5-year disease-specific survival ≥ 95%. In contrast, PCDLBCL, LT is considered an aggressive lymphoma with a survival rate in 5 years of lower than 60%. Patients with a solitary lesion or limited lesions in a single anatomical site require different treatments as compared to patients with generalized lesions or refractory disease or extracutaneous involvement. Therapeutic choice includes observation, local, or systemic therapy based on histology and disease extension. Patient management is multidisciplinary, including dermatologists, pathologists, hemato-oncologists, and radiation oncologists.
原发性皮肤B细胞淋巴瘤(PCBCL)是一组起源于B细胞的结外非霍奇金淋巴瘤,在诊断时主要累及皮肤,无皮肤外疾病证据。它们约占所有皮肤淋巴瘤的25%,分为三个主要亚组(世界卫生组织(WHO)2017年):原发性皮肤边缘区淋巴瘤(PCMZL)、原发性皮肤滤泡中心细胞淋巴瘤(PCFCL)和腿部弥漫性大B细胞淋巴瘤(PCDLBCL,LT)。该分类还包括一些不太常见的实体,如血管内大B细胞淋巴瘤。最近,WHO-EORTC将爱泼斯坦-巴尔病毒阳性(EBV+)黏膜皮肤溃疡作为一种新的临时独立实体纳入皮肤B细胞淋巴瘤。PCBCL的典型特征是斑块、斑片或结节,在颜色、形状和位置上具有很大的变异性。诊断需要进行组织学检查和免疫组化染色。一般来说,治疗方案取决于确切的组织学和免疫组化分类、疾病表现和风险评估。PCMZL和PCFCL被认为是惰性淋巴瘤,预后良好,5年疾病特异性生存率≥95%。相比之下,PCDLBCL,LT被认为是侵袭性淋巴瘤,5年生存率低于60%。与患有广泛性病变、难治性疾病或皮肤外受累的患者相比,患有单个病变或单个解剖部位局限性病变的患者需要不同的治疗方法。治疗选择包括根据组织学和疾病范围进行观察、局部或全身治疗。患者管理是多学科的,包括皮肤科医生、病理学家、血液肿瘤学家和放射肿瘤学家。