Fiorelli Alfonso, D'Andrilli Antonio, Carlucci Annalisa, Vicidomini Giovanni, Loizzi Domenico, Ardò Nicoletta Pia, Marasco Rita Daniela, Ventura Luigi, Ampollini Luca, Carbognani Paolo, Bocchialini Giovanni, Lococo Filippo, Paci Massimiliano, Di Stefano Teresa Severina, Ardissone Francesco, Gagliasso Matteo, Mendogni Paolo, Rosso Lorenzo, Mazzucco Alessandra, Vanni Camilla, Marinucci Beatrice Trabalza, Potenza Rossella, Matricardi Alberto, Ragusa Mark, Tassi Valentina, Anile Marco, Poggi Camilla, Serra Nicola, Sica Antonello, Nosotti Mario, Sollitto Francesco, Venuta Federico, Rendina Erino Angelo, Puma Francesco, Santini Mario
Translational Medical and Surgical Science, University of Campania Luigi Vanvitelli, Naples, Italy.
Thoracic Surgery, Università La Sapienza, Sant'Andrea Hospital, Rome, Italy.
Transl Lung Cancer Res. 2020 Feb;9(1):90-102. doi: 10.21037/tlcr.2019.12.28.
Second cancer is the leading cause of death in lymphoma survivors, with lung cancer representing the most common solid tumor. Limited information exists about the treatment and prognosis of second lung cancer following lymphoma. Herein, we evaluated the outcome and prognostic factors of Lung Cancer in Lymphoma Survivors (the LuCiLyS study) to improve the patient selection for lung cancer treatment.
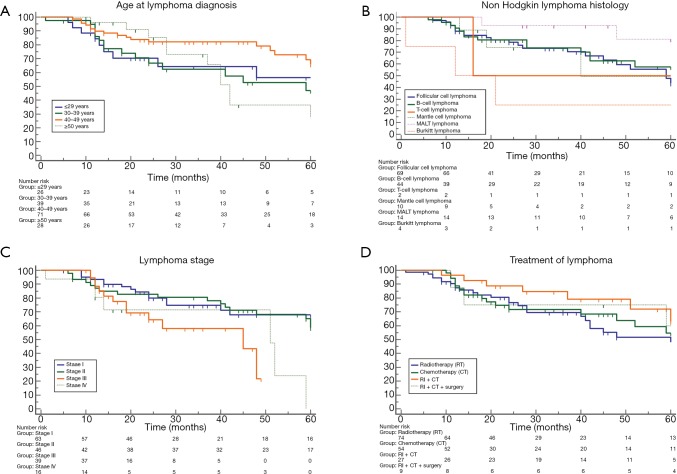
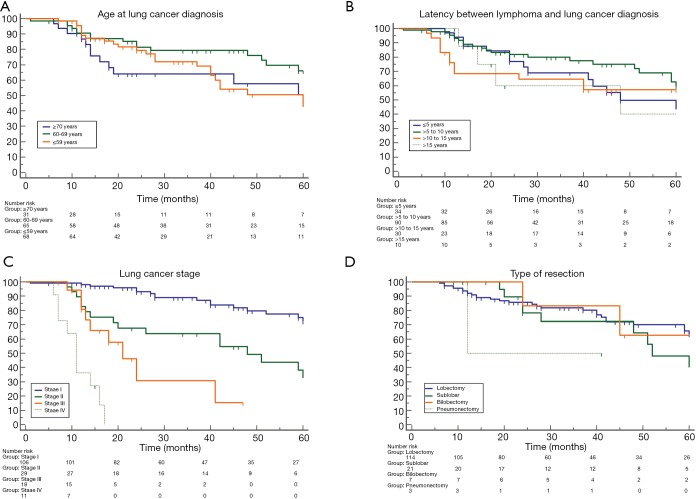
This is a retrospective multicentre study including consecutive patients treated for lymphoma disease that subsequently developed non-small cell lung cancer (NSCLC). Data regarding lymphoma including age, symptoms, histology, disease stage, treatment received and lymphoma status at the time of lung cancer diagnosis, and data on lung carcinoma as age, smoking history, latency from lymphoma, symptoms, histology, disease stage, treatment received, and survival were evaluated to identify the significant prognostic factors for overall survival.
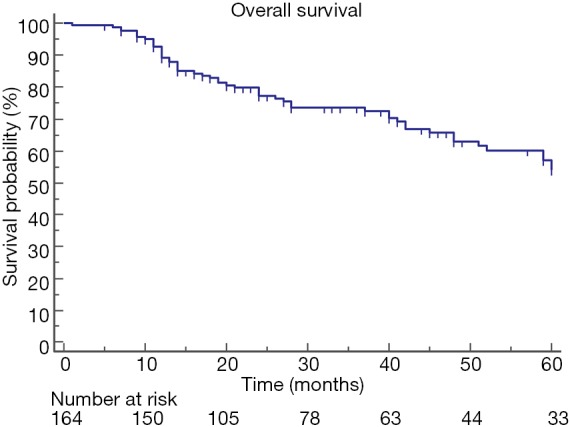
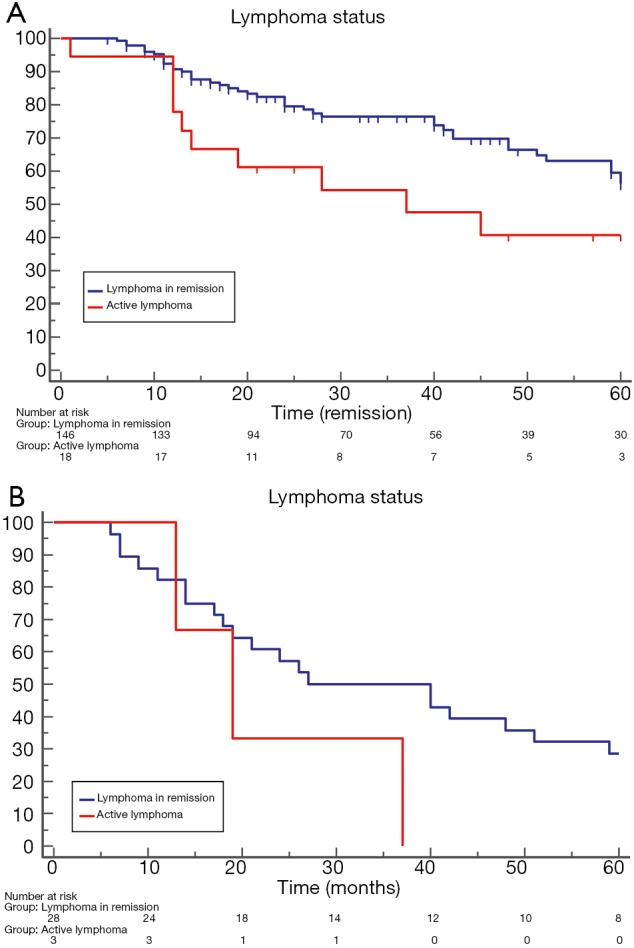
Our study population included 164 patients, 145 of which underwent lung cancer resection. The median overall survival was 63 (range, 58-85) months, and the 5-year survival rate 54%. At univariable analysis no-active lymphoma (HR: 2.19; P=0.0152); early lymphoma stage (HR: 1.95; P=0.01); adenocarcinoma histology (HR: 0.59; P=0.0421); early lung cancer stage (HR: 3.18; P<0.0001); incidental diagnosis of lung cancer (HR: 1.71; P<0.0001); and lung cancer resection (HR: 2.79; P<0.0001) were favorable prognostic factors. At multivariable analysis, no-active lymphoma (HR: 2.68; P=0.004); early lung cancer stage (HR: 2.37; P<0.0001); incidental diagnosis of lung cancer (HR: 2.00; P<0.0001); and lung cancer resection (HR: 2.07; P<0.0001) remained favorable prognostic factors. Patients with non-active lymphoma (n=146) versus those with active lymphoma (n=18) at lung cancer diagnosis presented better median survival (64 37 months; HR: 2.4; P=0.02), but median lung cancer specific survival showed no significant difference (27 19 months; HR: 0.3; P=0.17).
The presence and/or a history of lymphoma should not be a contraindication to resection of lung cancer. Inclusion of lymphoma survivors in a lung cancer-screening program may lead to early detection of lung cancer, and improve the survival.
第二原发癌是淋巴瘤幸存者的主要死因,肺癌是最常见的实体瘤。关于淋巴瘤后第二原发肺癌的治疗和预后信息有限。在此,我们评估了淋巴瘤幸存者肺癌的结局和预后因素,以改善肺癌治疗的患者选择。
这是一项回顾性多中心研究,纳入了连续接受淋巴瘤治疗且随后发生非小细胞肺癌(NSCLC)的患者。评估了包括年龄、症状、组织学、疾病分期、肺癌诊断时接受的治疗和淋巴瘤状态等淋巴瘤相关数据,以及包括年龄、吸烟史、淋巴瘤发病至肺癌的间隔时间、症状、组织学、疾病分期、接受的治疗和生存情况等肺癌相关数据,以确定总生存的显著预后因素。
我们的研究队列包括164例患者,其中145例行肺癌切除术。中位总生存时间为63(范围58 - 85)个月,5年生存率为54%。单因素分析显示,无活动期淋巴瘤(HR:2.19;P = 0.0152)、淋巴瘤早期阶段(HR:1.95;P = 0.01)、腺癌组织学(HR:0.59;P = 0.0421)、肺癌早期阶段(HR:3.18;P < 0.0001)、肺癌偶然诊断(HR:1.71;P < 0.0001)和肺癌切除术(HR:2.79;P < 0.0001)是有利的预后因素。多因素分析显示,无活动期淋巴瘤(HR:2.68;P = 0.004)、肺癌早期阶段(HR:2.37;P < 0.0001)、肺癌偶然诊断(HR:2.00;P < 0.0001)和肺癌切除术(HR:2.07;P < 0.0001)仍是有利的预后因素。肺癌诊断时无活动期淋巴瘤患者(n = 146)与有活动期淋巴瘤患者(n = 18)相比,中位生存时间更长(64对37个月;HR:2.4;P = 0.02),但肺癌特异性中位生存时间无显著差异(27对19个月;HR:0.3;P = 0.17)。
淋巴瘤的存在和/或病史不应成为肺癌切除的禁忌证。将淋巴瘤幸存者纳入肺癌筛查计划可能会导致肺癌的早期发现,并改善生存。