Albach Fredrik N, Geier Christian, Keicher Christian, Posch Maximilian G, Schreiber Stephan J, Grütz Gerald, Akyüz Levent, Luo Xiaodong, Le-Halpere Annaig, Truffinet Philippe, Wagner Frank
Charité Research Organisation GmbH, Berlin, Germany.
Department of Neurology, Oberhavel Clinic, Henningsdorf, Germany.
Neurol Ther. 2024 Dec;13(6):1607-1625. doi: 10.1007/s40120-024-00659-w. Epub 2024 Sep 9.
Lymphocyte depletion via anti-CD52 monoclonal antibody (mAb) therapy is an effective treatment strategy for relapsing-remitting multiple sclerosis (MS) but is associated with infusion/injection-associated reactions (IARs) and autoimmune-related adverse events (AEs). Gatralimab is a next-generation humanized anti-CD52 mAb.
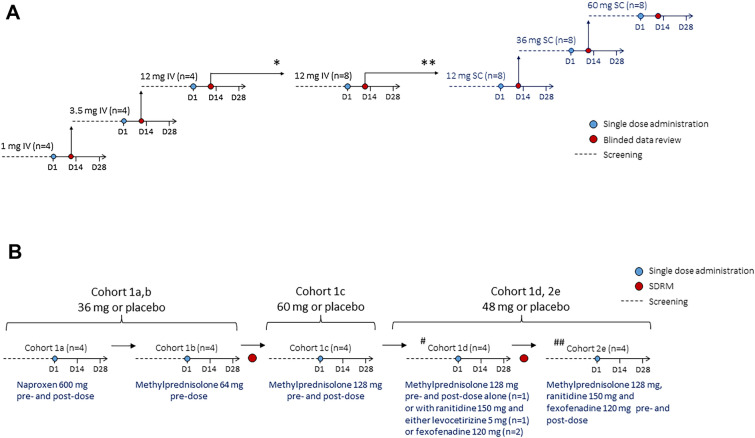
Two first-in-human trials were conducted in participants with progressive MS to assess the pharmacodynamics, pharmacokinetics, and safety of gatralimab administered via subcutaneous (SC) and intravenous (IV) routes, and to determine the effect of different comedication regimes on IARs to SC gatralimab. A Phase 1 trial (NCT02282826) included double-blind, placebo-controlled sequential ascending single IV (1, 3.5, and 12 mg) and SC (12, 36, and 60 mg) dose groups. A Phase 1b trial (NCT02977533) involved five groups who received SC gatralimab (36, 48, or 60 mg) and different comedications. A long-term safety (LTS) study (NCT02313285) examined safety and pharmacodynamics over 4 years.
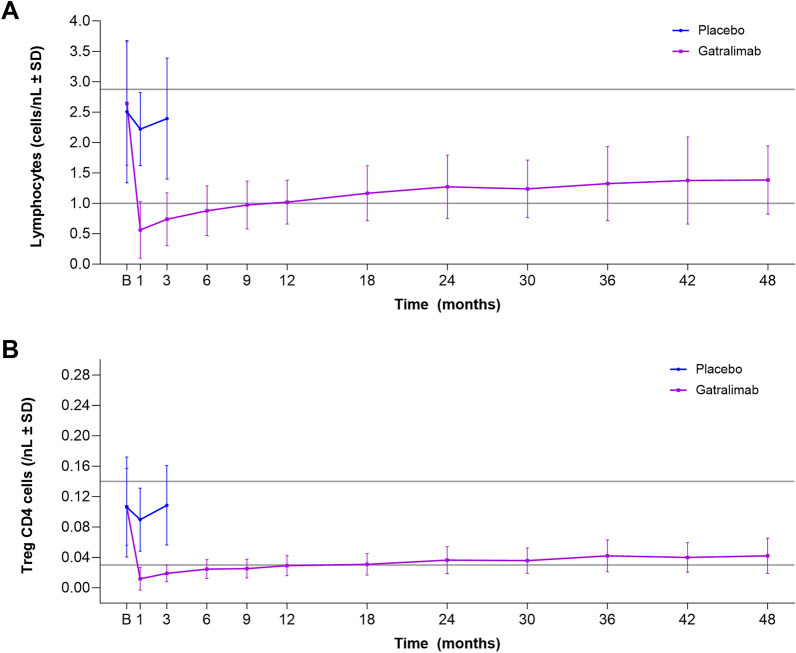
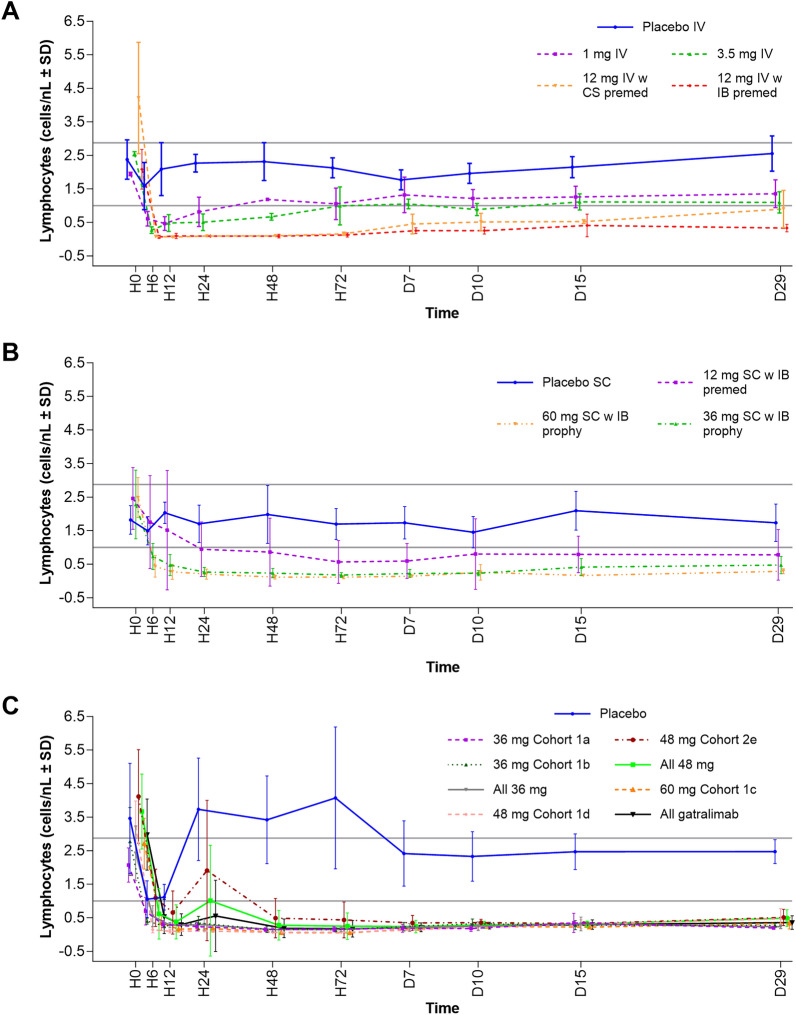
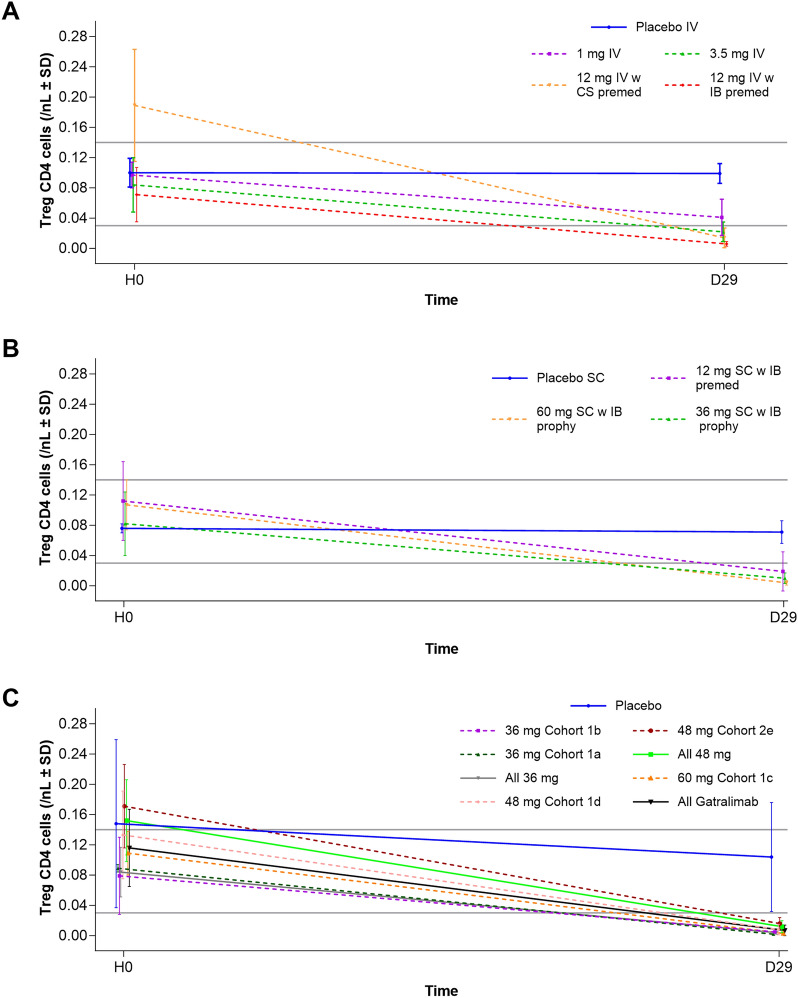
Gatralimab produced depletion of lymphocytes (dose-dependently) and CD4+ regulatory T cells, with partial repopulation to normal values by approximately 12 months. Peak serum gatralimab concentrations followed dose-proportionality and were delayed by 6.0-7.5 days following SC administration. Treatment-emergent AEs, including IARs, were reported for most participants but were generally of mild or moderate severity, and treatment-emergent serious AEs were mostly MS-related. Methylprednisolone and antihistamine comedications were associated with reduced incidence of fevers and skin and subcutaneous tissue AEs, respectively. During the LTS study, one participant (3.0%) experienced an autoimmune-related AE (Basedow's disease), and subsequently died from pulmonary sepsis deemed unrelated to gatralimab by the investigator.
These data show that gatralimab achieves the desired pharmacodynamic effect of lymphocyte depletion followed by repopulation, and has an acceptable safety profile, including low risk of non-MS autoimmunity. Although gatralimab is no longer in development for MS, insights from these trials may inform the development of comedication regimes of future anti-CD52 mAbs and subcutaneous formulations of other lymphocyte-depleting mAbs.
NCT02282826, NCT02977533, NCT02313285.
通过抗CD52单克隆抗体(mAb)疗法进行淋巴细胞清除是复发缓解型多发性硬化症(MS)的一种有效治疗策略,但与输注/注射相关反应(IARs)和自身免疫相关不良事件(AEs)有关。加曲利单抗是一种新一代人源化抗CD52 mAb。
在进行性MS患者中开展了两项首次人体试验,以评估通过皮下(SC)和静脉(IV)途径给药的加曲利单抗的药效学、药代动力学和安全性,并确定不同联合用药方案对SC加曲利单抗IARs的影响。一项1期试验(NCT02282826)包括双盲、安慰剂对照的序贯递增单次IV(1、3.5和12 mg)和SC(12、36和60 mg)剂量组。一项1b期试验(NCT02977533)涉及五组接受SC加曲利单抗(36、48或60 mg)和不同联合用药的患者。一项长期安全性(LTS)研究(NCT02313285)在4年时间里对安全性和药效学进行了研究。
加曲利单抗导致淋巴细胞(呈剂量依赖性)和CD4+调节性T细胞耗竭,约12个月后部分恢复至正常值。血清加曲利单抗峰值浓度呈剂量比例关系,SC给药后延迟6.0 - 7.5天出现。大多数参与者报告了包括IARs在内的治疗中出现的AE,但一般为轻度或中度严重程度,治疗中出现的严重AE大多与MS相关。甲基强的松龙和抗组胺联合用药分别与发热及皮肤和皮下组织AE的发生率降低相关。在LTS研究期间,一名参与者(3.0%)发生了自身免疫相关AE(巴塞多病),随后死于调查人员认为与加曲利单抗无关的肺部败血症。
这些数据表明,加曲利单抗实现了淋巴细胞耗竭后再填充的预期药效学效果,并且具有可接受的安全性,包括非MS自身免疫的低风险。尽管加曲利单抗不再针对MS进行研发,但这些试验的见解可能为未来抗CD52 mAbs联合用药方案及其他淋巴细胞清除mAbs皮下制剂的研发提供参考。
NCT02282826、NCT02977533、NCT02313285。