Department of Health and Care Sciences, UiT The Arctic University of Norway, Postboks 6050 Langnes, 9037, Tromsø, Norway.
Institute of Neuroscience and Physiology, Department of Clinical Neuroscience, Rehabilitation Medicine, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden.
J Neuroeng Rehabil. 2020 Jun 15;17(1):76. doi: 10.1186/s12984-020-00705-2.
Reduction of compensation and improved movement quality indicate recovery after stroke. Since clinical measures alone are often inadequate to distinguish between behavioral recovery and compensation, kinematic analysis of functional tasks has been recommended.
To quantify longitudinal changes and residual deficits in movement performance and quality during the first year after stroke using kinematic analysis of drinking task.
A total of 56 participants with first ever stroke causing upper extremity impairment were extracted from a non-selected stroke unit cohort (Stroke Arm Longitudinal Study at the University of Gothenburg-SALGOT). Participants needed to able to perform the drinking task with the more-affected arm at least on 2 occasions out of 6 (3 days, 10 days, 4 weeks, and 3, 6, and 12 months) during the first year to be included. A cohort of 60 healthy individuals was used as reference. Longitudinal changes were analyzed using linear mixed models.
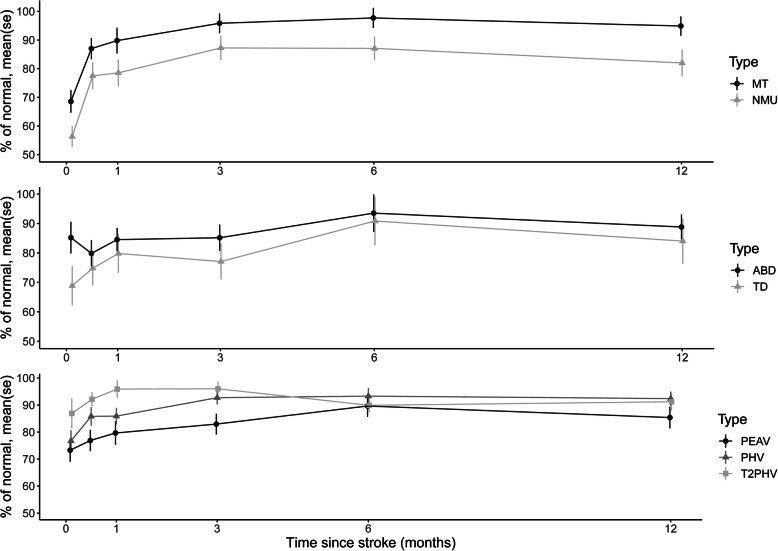
Movement time, number of movement units, peak angular velocity of the elbow, peak hand velocity, and trunk displacement improved significantly over the first 3 months with a peak at 6 months. Movement time and peak hand velocity reached levels comparable to healthy at 3 months, but number of movement units, peak elbow angular velocity, trunk displacement, and arm abduction remained different from healthy over the first year after stroke.
Even when the recovery patterns of kinematics follow the known nonlinear pattern, not all kinematic measures reach the levels in par with healthy controls at one year post stroke. Since the number of movement units, peak angular velocity, trunk displacement, and arm abduction remained impaired over the first year, they might be the most suited measures to distinguish behavioral recovery from compensation strategies.
ClinicalTrials: NCT01115348. 4 May 2010. Retrospectively registered.
减少补偿和提高运动质量表明中风后康复。由于仅临床措施往往不足以区分行为恢复和补偿,因此推荐对功能任务的运动学进行分析。
使用饮水任务的运动学分析,量化中风后第一年运动表现和质量的纵向变化和残留缺陷。
从哥德堡大学非选择性中风病房队列(哥德堡大学中风手臂纵向研究-SALGOT)中提取了 56 名首次中风导致上肢受损的参与者。参与者需要在第一年的 6 次(3 天、10 天、4 周以及 3、6 和 12 个月)中至少有 2 次能够用患侧手臂完成饮水任务,才能被纳入研究。一个由 60 名健康个体组成的队列被用作参考。使用线性混合模型分析纵向变化。
运动时间、运动单元数、肘部峰值角速度、手部峰值速度和躯干位移在头 3 个月内显著改善,在 6 个月时达到峰值。运动时间和手部峰值速度在 3 个月时达到与健康人相当的水平,但运动单元数、肘部峰值角速度、躯干位移和手臂外展仍在中风后 1 年内与健康人不同。
即使运动学的恢复模式遵循已知的非线性模式,并非所有运动学测量值在中风后 1 年都能达到与健康对照组相当的水平。由于运动单元数、峰值角速度、躯干位移和手臂外展在第一年仍存在损伤,因此它们可能是区分行为恢复和补偿策略的最适合的指标。
ClinicalTrials.gov:NCT01115348。2010 年 5 月 4 日。回顾性注册。