Kim Yong-Il, Yoo Changhoon, Oh Seung Jun, Lee Sang Ju, Kang Junho, Hwang Hee-Sang, Hong Seung-Mo, Ryoo Baek-Yeol, Ryu Jin-Sook
Department of Nuclear Medicine, Asan Medical Center, University of Ulsan College of Medicine, 88, Olympic-ro 43-gil, Songpa-gu, Seoul, 05505, Republic of Korea.
Department of Oncology, Asan Medical Center, University of Ulsan College of Medicine, 88, Olympic-ro 43-gil, Songpa-gu, Seoul, 05505, Republic of Korea.
EJNMMI Res. 2020 Jun 15;10(1):63. doi: 10.1186/s13550-020-00651-z.
Lanreotide is a long-acting somatostatin analogue with proven antitumour effects against well-differentiated (WD) gastroenteropancreatic-neuroendocrine tumours (GEP-NETs). However, there are no globally established prognostic factors associated with the efficacy of lanreotide as a treatment for GEP-NETs. We investigated the prognostic value of [Ga]Ga-DOTA-TOC positron emission tomography (PET)/computed tomography (CT) somatostatin receptor imaging for patients with WD GEP-NETs treated with lanreotide.
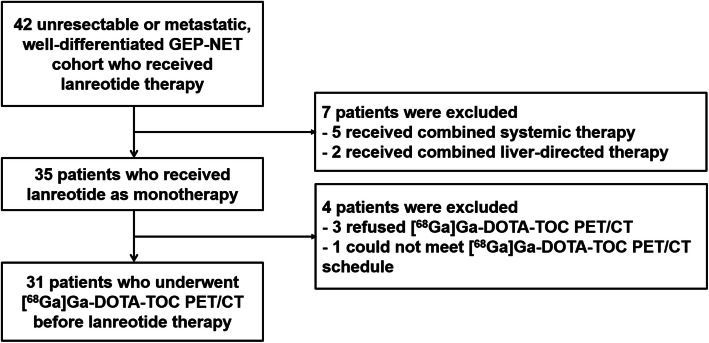
In this retrospective study, we included 31 patients with unresectable or metastatic WD GEP-NETs who received lanreotide and underwent [Ga]Ga-DOTA-TOC PET/CT before receiving lanreotide. We captured the following clinicopathological variables: Eastern Cooperative Oncology Group (ECOG) performance status, primary tumour site, NET World Health Organization grade, existence of carcinoid symptoms, previous surgery, previous chemotherapy, and hepatic tumour volume assessed by CT or magnetic resonance imaging (MRI). We also assessed the following [Ga]Ga-DOTA-TOC PET/CT variables: Krenning score, tumour-to-liver ratio (TLR), maximum standardized uptake value (SUVmax), whole tumour volume (WTV), and total receptor expression (TRE, WTV multiplied by SUVmean). The associations between these markers and progression-free survival (PFS) with lanreotide were analysed.
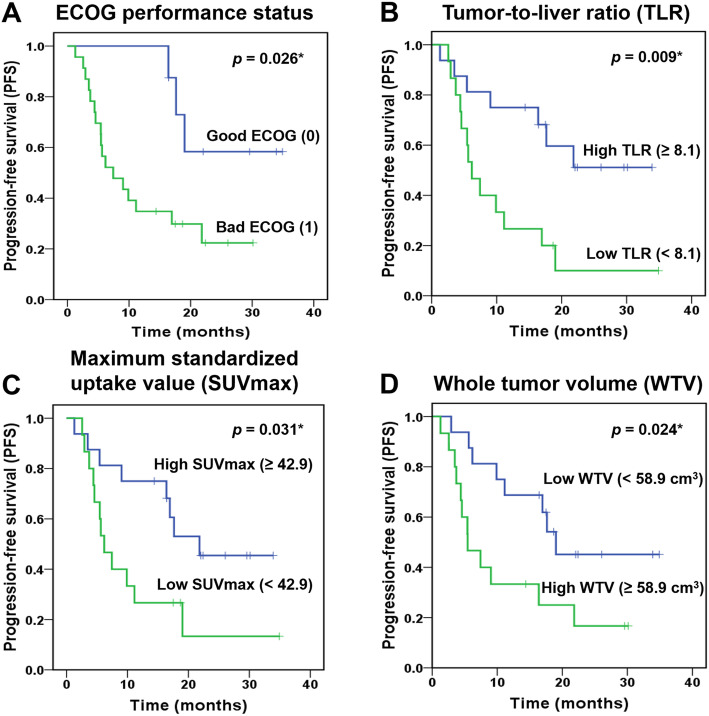
The mean age was 55.1 ± 15.5 years (range 16.0-81.0). The most common primary tumour site was the pancreas, followed by the stomach, and rectum. The median PFS interval with lanreotide was 14.4 months (range 1.3-34.9), with identified disease progression in 20 patients (64.5%). Among the [Ga]Ga-DOTA-TOC PET/CT variables, TLR (< 8.1 vs. ≥ 8.1; p = 0.013), SUVmax (< 42.9 vs. ≥ 42.9; p = 0.037), and WTV (≥ 58.9 cm vs. < 58.9 cm; p = 0.030) were significantly associated with PFS in the univariate analyses, but only TLR (hazard ratio 3.182 [95% CI 1.189-8.514], p = 0.021) remained an independent factor for PFS in the multivariate analysis.
Low TLR, determined via [Ga]Ga-DOTA-TOC PET/CT, can be a factor of worse prognosis in patients with advanced WD GEP-NETs treated with lanreotide.
兰瑞肽是一种长效生长抑素类似物,已证实对高分化(WD)胃肠胰神经内分泌肿瘤(GEP-NETs)具有抗肿瘤作用。然而,目前尚无全球公认的与兰瑞肽治疗GEP-NETs疗效相关的预后因素。我们研究了[镓]Ga-DOTA-TOC正电子发射断层扫描(PET)/计算机断层扫描(CT)生长抑素受体显像对接受兰瑞肽治疗的WD GEP-NETs患者的预后价值。
在这项回顾性研究中,我们纳入了31例不可切除或转移性WD GEP-NETs患者,这些患者接受了兰瑞肽治疗,并在接受兰瑞肽治疗前进行了[镓]Ga-DOTA-TOC PET/CT检查。我们记录了以下临床病理变量:东部肿瘤协作组(ECOG)体能状态、原发肿瘤部位、NET世界卫生组织分级、类癌症状的存在情况、既往手术史、既往化疗史以及通过CT或磁共振成像(MRI)评估的肝肿瘤体积。我们还评估了以下[镓]Ga-DOTA-TOC PET/CT变量:克伦宁评分、肿瘤与肝脏比值(TLR)、最大标准化摄取值(SUVmax)、全肿瘤体积(WTV)以及总受体表达(TRE,WTV乘以SUVmean)。分析了这些标志物与兰瑞肽治疗的无进展生存期(PFS)之间的关联。
平均年龄为55.1±15.5岁(范围16.0 - 81.0岁)。最常见的原发肿瘤部位是胰腺,其次是胃和直肠。兰瑞肽治疗的中位PFS间隔为14.4个月(范围1.3 - 34.9个月),20例患者(64.5%)出现疾病进展。在[镓]Ga-DOTA-TOC PET/CT变量中,单因素分析显示TLR(<8.1 vs.≥8.1;p = 0.013)、SUVmax(<42.9 vs.≥42.9;p = 0.037)和WTV(≥58.9 cm vs.<58.9 cm;p = 0.030)与PFS显著相关,但多因素分析中只有TLR(风险比3.182 [95% CI 1.189 - 8.514],p = 0.021)仍然是PFS的独立因素。
通过[镓]Ga-DOTA-TOC PET/CT测定的低TLR可能是接受兰瑞肽治疗的晚期WD GEP-NETs患者预后较差的一个因素。