Department of Cardiology, The First Affiliated Hospital of Sun Yat-Sen University, Guangzhou, China.
NHC Key Laboratory of Assisted Circulation (Sun Yat-sen University), Guangzhou, China.
J Diabetes Investig. 2021 Jan;12(1):99-108. doi: 10.1111/jdi.13324. Epub 2020 Jul 26.
AIMS/INTRODUCTION: To appraise guidelines on the antiplatelet strategy of prevention of cardiovascular disease (CVD) in patients with type 2 diabetes mellitus, and highlight the consensuses and controversies to aid clinician decision-making.
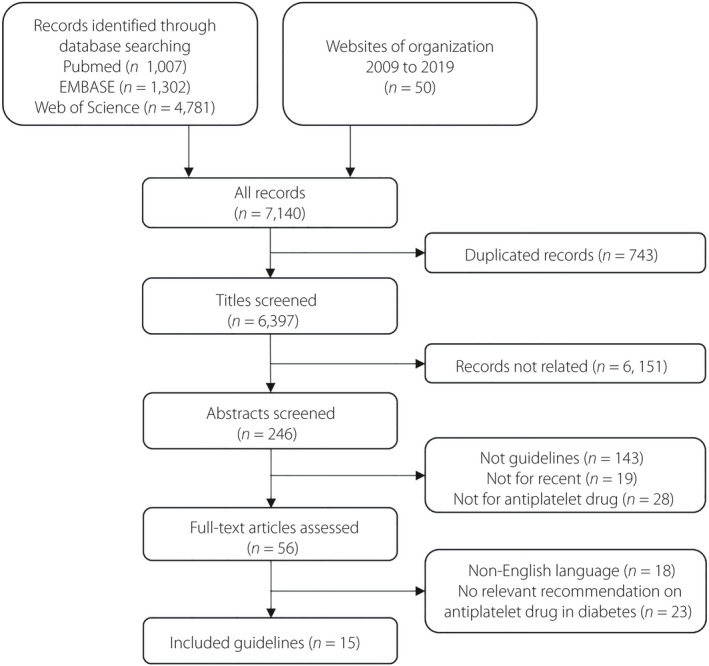
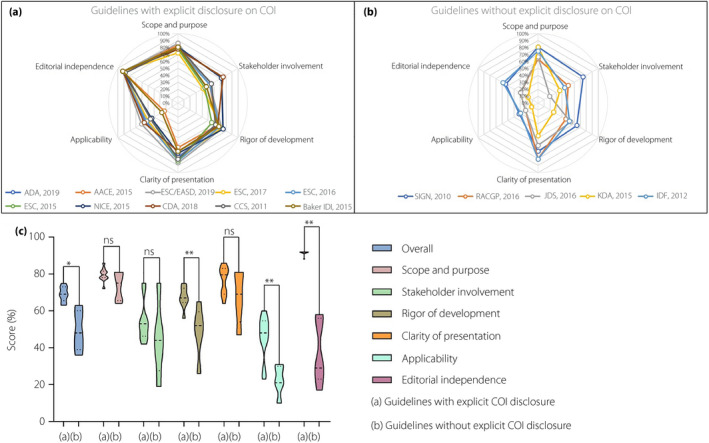
A systematic search was carried out for guidelines regarding CVD prevention or focusing on type 2 diabetes patients. Appraisal of Guidelines for Research and Evaluation II instrument was utilized to appraise the quality of included guidelines.
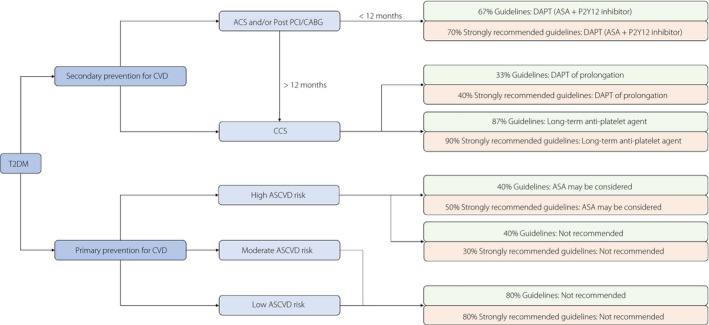
Of the 15 guidelines with discrepant Appraisal of Guidelines for Research and Evaluation II scores (66%; interquartile range 51-71%), 10 were defined as "strongly recommended" guidelines. For secondary prevention, >60% of guidelines advocated that the dual antiplatelet therapy was used within 12 months when the type 2 diabetes patients experienced acute coronary syndrome and/or post-percutaneous coronary intervention or coronary artery bypass grafting, with subsequent long-term aspirin use. For primary prevention, 80% of guidelines supported that aspirin should not be routinely used by patients with type 2 diabetes. No consensus on whether to prolong dual antiplatelet therapy in secondary prevention, and whether to use aspirin in type 2 diabetes patients with high CVD risk exists in current guidelines.
Physicians should use the recommendations from "strongly recommended" guidelines to make informed decisions and know the consensuses of current guidelines. Dual antiplatelet therapy should be used within 12 months when type 2 diabetes patients experience acute coronary syndrome and/or percutaneous coronary intervention/coronary artery bypass grafting, with subsequent long-term aspirin use. In primary prevention, aspirin should not be routinely used by individuals with type 2 diabetes, but might be considered for those with high CVD risk.
目的/引言:评估关于 2 型糖尿病患者心血管疾病(CVD)预防的抗血小板策略指南,并强调共识和争议,以帮助临床医生做出决策。
对预防 CVD 或专注于 2 型糖尿病患者的指南进行了系统搜索。使用评估指南研究和评估 II 工具来评估纳入指南的质量。
在存在差异的 15 项指南中(66%;四分位间距为 51-71%),有 10 项被定义为“强烈推荐”指南。对于二级预防,超过 60%的指南主张在 2 型糖尿病患者经历急性冠脉综合征和/或经皮冠状动脉介入治疗或冠状动脉旁路移植术后的 12 个月内使用双联抗血小板治疗,随后长期使用阿司匹林。对于一级预防,80%的指南支持 2 型糖尿病患者不应常规使用阿司匹林。目前的指南中没有关于是否在二级预防中延长双联抗血小板治疗以及在 CVD 风险高的 2 型糖尿病患者中使用阿司匹林的共识。
医生应使用“强烈推荐”指南中的建议做出明智的决策,并了解当前指南的共识。在 2 型糖尿病患者经历急性冠脉综合征和/或经皮冠状动脉介入治疗/冠状动脉旁路移植术后,应在 12 个月内使用双联抗血小板治疗,随后长期使用阿司匹林。在一级预防中,2 型糖尿病患者不应常规使用阿司匹林,但对于 CVD 风险高的患者,可以考虑使用。