University of Utah, College of Nursing, 10 2000 E, Salt Lake City, UT 84112. Email:
University of Utah, College of Nursing, Salt Lake City, Utah.
Prev Chronic Dis. 2020 Jun 18;17:E45. doi: 10.5888/pcd17.190339.
Emergency departments see a disproportionate share of low-income and uninsured patients. We developed and evaluated a process for identifying social needs among emergency department patients, for facilitating access to community-based resources, and for integrating clinical and community-based data.
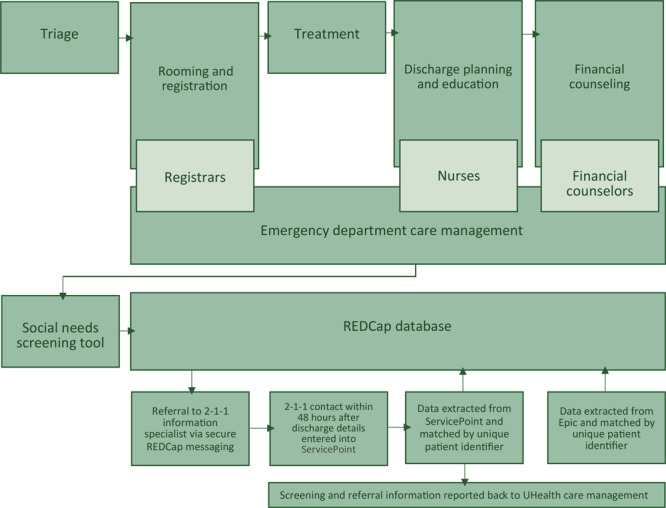
We leveraged an academic-community partnership to develop a social needs screening tool and referral process.
In a 25-day feasibility trial incorporating rapid improvement cycles, emergency department staff screened 210 patients for social needs. Observational and interview notes were analyzed, and data were linked from patient screenings, the United Way of Salt Lake 2-1-1 consumer information system, and electronic health records.
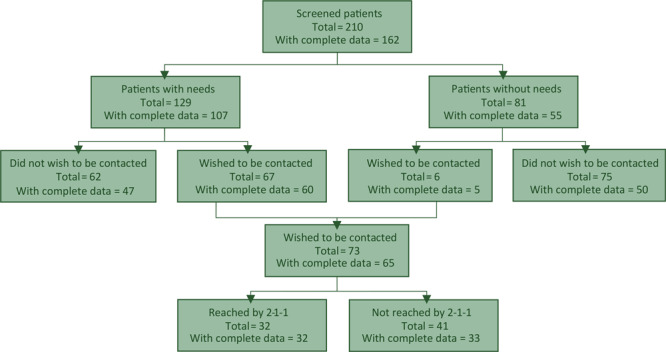
Domains uncovered during pilot testing included screening based on appearance or insurance; discomfort asking stigmatizing questions; and lack of clarity regarding the screening's purpose. During the trial, 61% (n = 129) of patients reported 1 or more need, 52% (n = 67) of whom wanted follow-up. Of the 65 patients with complete data who wanted referrals, 49% (n = 32) were ultimately reached by 2-1-1, which provided an average of 4 community referrals (eg, pharmacy programs, utility assistance). Service usage 3 months before versus 3 months after emergency department index dates demonstrated that patients with social needs experienced a significant increase in emergency department use compared with those without needs (1.07 vs 1.36, P = .03), while patients with no needs experienced increases in primary care visits compared with those patients with unmet needs (0.24 vs 0.56, P = .03).
We demonstrated the ability to systematically screen and refer for emergency department patients' unmet social needs by using existing resources and to link screening results, service referral details, and health service data. However, our experiences demonstrate that widespread implementation efforts should thoughtfully address staff perceptions and patient communication challenges.
急诊科接诊了大量低收入和无保险患者。我们开发并评估了一种识别急诊科患者社会需求的方法,以促进获得基于社区的资源,并整合临床和基于社区的数据。
我们利用学术-社区伙伴关系开发了一种社会需求筛查工具和转介流程。
在一项为期 25 天的可行性试验中,我们纳入了快速改进循环,急诊工作人员对 210 名患者进行了社会需求筛查。对观察和访谈记录进行了分析,并将患者筛查、联合之路盐湖城 2-1-1 消费者信息系统和电子健康记录的数据进行了关联。
试点测试中发现的领域包括基于外观或保险进行筛查;不愿询问有污名的问题;以及对筛查目的不清楚。在试验期间,61%(n=129)的患者报告了 1 项或多项需求,其中 52%(n=67)的患者希望跟进。在有完整数据且希望转介的 65 名患者中,有 49%(n=32)最终通过 2-1-1 联系上,该系统提供了平均 4 个社区转介(如药房项目、水电费援助)。在急诊指数日期前 3 个月和后 3 个月的服务使用情况显示,有社会需求的患者与无需求的患者相比,急诊就诊次数显著增加(1.07 比 1.36,P=0.03),而无需求的患者与未满足需求的患者相比,初级保健就诊次数增加(0.24 比 0.56,P=0.03)。
我们通过使用现有资源,展示了为急诊科患者未满足的社会需求进行系统筛查和转介的能力,并将筛查结果、服务转介细节和卫生服务数据进行了关联。然而,我们的经验表明,广泛的实施工作应该认真解决员工的看法和患者沟通方面的挑战。