Oncology, Johns Hopkins Medicine Sidney Kimmel Comprehensive Cancer Center, Baltimore, Maryland, USA
The Bloomberg~Kimmel Institute for Cancer Immunotherapy, Johns Hopkins University, Baltimore, Maryland, USA.
J Immunother Cancer. 2020 Jun;8(1). doi: 10.1136/jitc-2020-000840.
Pneumonitis from immune checkpoint inhibitors (ICI) is a potentially fatal immune-related adverse event (irAE) from antiprogrammed death 1/programmed death ligand 1 immunotherapy. Most cases of ICI pneumonitis improve or resolve with 4-6 weeks of corticosteroid therapy. Herein, we report the incidence, clinicopathological features and management of patients with non-small cell lung cancer (NSCLC) and melanoma who developed chronic ICI pneumonitis that warrants ≥12 weeks of immunosuppression.
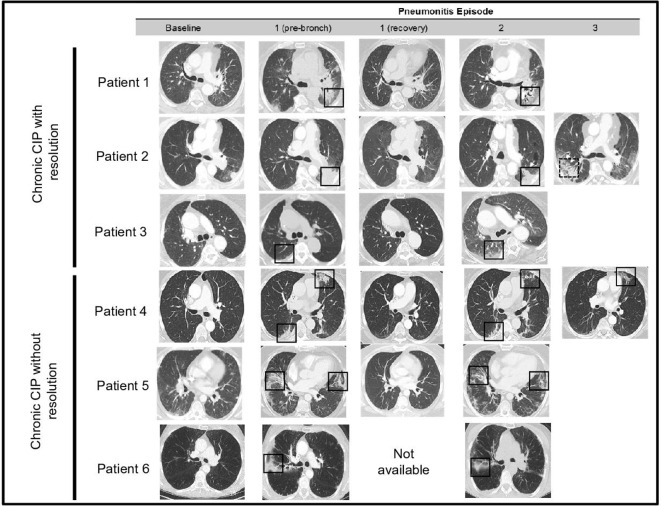
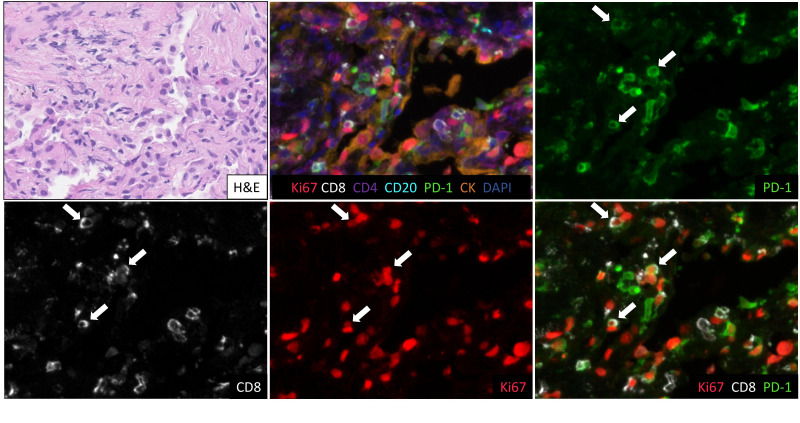
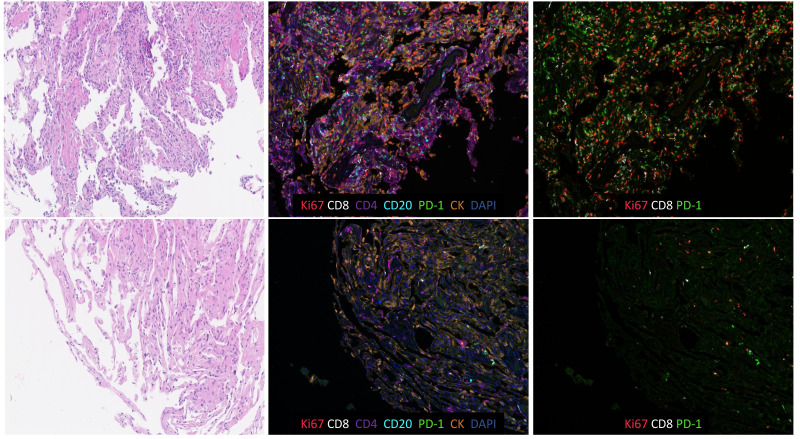
Patients with ICI pneumonitis were identified from institutional databases of ICI-treated patients with advanced melanoma and NSCLC between January 2011 and July 2018. ICI pneumonitis was defined as clinical/radiographic evidence of lung inflammation without alternative diagnoses, adjudicated by a multidisciplinary team. Chronic ICI pneumonitis was defined as pneumonitis that persists or worsens with steroid tapering, and necessitates ≥12 weeks of immunosuppression, after ICI discontinuation. Serial chest CT was used to assess radiological features, and tumor response by Response EvaluationCriteria for Solid Tumors V.1.1. Bronchoalveolar lavage fluid (BALF) samples were assessed by cell differential. Lung biopsy samples were evaluated by H&E staining and multiplex immunofluorescence (mIF), where available.
Among 299 patients, 44 developed ICI pneumonitis (NSCLC: 5/205; melanoma: 1/94), and of these, 6 experienced chronic ICI pneumonitis. The overall incidence of chronic ICI pneumonitis was thus 2%. Of those who developed chronic ICI pneumonitis: the majority had NSCLC (5/6), all sustained disease control from ICIs, and none had other concurrent irAEs. Timing of chronic ICI pneumonitis development was variable (range: 0-50 months), and occurred at a median of 12 months post ICI start. Recrudescence of ICI pneumonitis occurred at a median of 6 weeks after initial steroid start (range: 3-12 weeks), with all patients requiring steroid reintroduction when tapered to ≤10 mg prednisone/equivalent. The median total duration of steroids was 37 weeks (range: 16-43+weeks). Re-emergence of radiographic ICI pneumonitis occurred in the same locations on chest CT, in most cases (5/6). All patients who developed chronic ICI pneumonitis had BALF lymphocytosis on cell differential and organising pneumonia on lung biopsy at initial ICI pneumonitis presentation, with persistent BALF lymphocytosis and brisk CD8+ infiltration on mIF at pneumonitis re-emergence during steroid taper.
A subset of patients who develop pneumonitis from ICIs will develop chronic ICI pneumonitis, that warrants long-term immunosuppression of ≥12 weeks, and has distinct clinicopathological features.
免疫检查点抑制剂(ICI)引起的肺炎是抗程序性死亡 1/程序性死亡配体 1 免疫治疗引起的潜在致命免疫相关不良事件(irAE)。大多数 ICI 性肺炎在接受皮质类固醇治疗 4-6 周后可改善或缓解。在此,我们报告了在接受抗程序性死亡 1/程序性死亡配体 1 免疫治疗的晚期黑色素瘤和非小细胞肺癌(NSCLC)患者中发生的需要 12 周以上免疫抑制治疗的慢性 ICI 性肺炎的发生率、临床病理特征和处理方法。
从 2011 年 1 月至 2018 年 7 月接受 ICI 治疗的晚期黑色素瘤和 NSCLC 患者的机构数据库中确定了发生 ICI 性肺炎的患者。ICI 性肺炎的定义为临床/影像学有肺部炎症的证据,无其他诊断,由多学科团队判定。慢性 ICI 性肺炎的定义为在 ICI 停药后,随着皮质类固醇的减量,肺炎持续或恶化,需要≥12 周的免疫抑制治疗。连续胸部 CT 用于评估影像学特征和实体瘤反应评价标准 1.1 版(Response Evaluation Criteria for Solid Tumors V.1.1)对肿瘤反应的评估。支气管肺泡灌洗液(BALF)样本通过细胞差异评估。肺活检样本通过 H&E 染色和多重免疫荧光(mIF)评估,如适用。
在 299 名患者中,44 名患者发生 ICI 性肺炎(NSCLC:5/205;黑色素瘤:1/94),其中 6 名患者发生慢性 ICI 性肺炎。因此,慢性 ICI 性肺炎的总发生率为 2%。发生慢性 ICI 性肺炎的患者中:大多数为 NSCLC(5/6),所有患者均从 ICI 中获得持续的疾病控制,且无其他同时发生的 irAE。慢性 ICI 性肺炎的发病时间各不相同(范围:0-50 个月),中位发病时间为 ICI 开始后 12 个月。在初始类固醇开始后 6 周(范围:3-12 周)出现 ICI 性肺炎复发,所有患者在减至≤10 mg 泼尼松/等效物时需要重新开始使用类固醇。类固醇的总持续时间中位数为 37 周(范围:16-43+周)。在胸部 CT 上,在大多数情况下(5/6),在同一部位出现 ICI 性肺炎的影像学复发。在最初的 ICI 性肺炎发作时,所有发生慢性 ICI 性肺炎的患者的 BALF 细胞差异均有淋巴细胞增多,肺活检均有组织性肺炎,在类固醇减量期间出现 ICI 性肺炎复发时,BALF 淋巴细胞增多和 CD8+浸润明显。
从 ICI 发展而来的肺炎的一部分患者将发展为慢性 ICI 性肺炎,需要≥12 周的长期免疫抑制治疗,并且具有独特的临床病理特征。