Arango-Granados María Camila, Cruz Mendoza Diego Fernando, Salcedo Cadavid Alexander Ernesto, García Marín Alberto Federico
Fundación Valle del Lili, Cra. 98 ## 18-49, Cali, Valle del Cauca, Colombia; Universidad Icesi, Cl. 18 #122-135, Facultad de Medicina, Cali, Valle del Cauca, Colombia.
Int J Surg Case Rep. 2020;72:346-350. doi: 10.1016/j.ijscr.2020.05.087. Epub 2020 Jun 12.
Crush syndrome (CS) is a condition with a high morbidity and mortality due to severe electrolyte disorders, circulatory dysfunction and multiple organ failure, secondary to severe rhabdomyolysis and reperfusion injuries. There is controversy about the role of fasciotomy in the treatment of compartment syndromes due to crush injuries and it is still unknown if early amputation has patient-centered benefits.
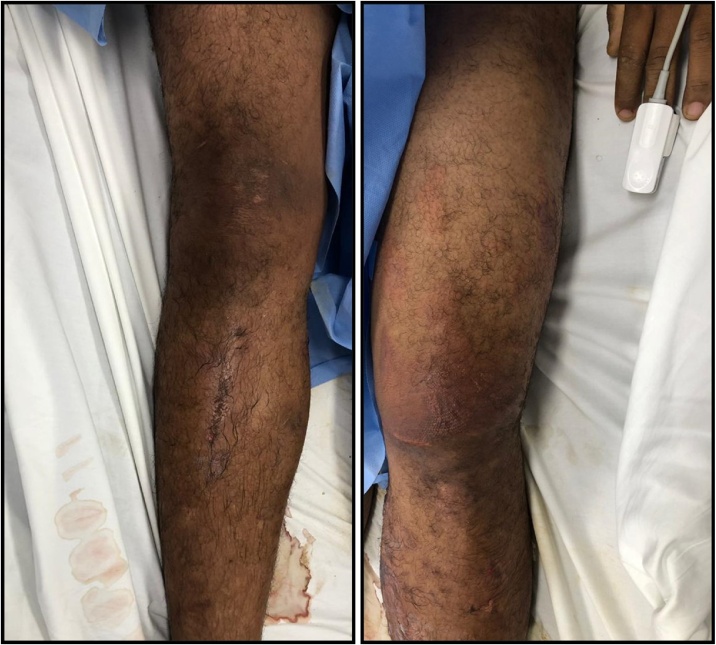
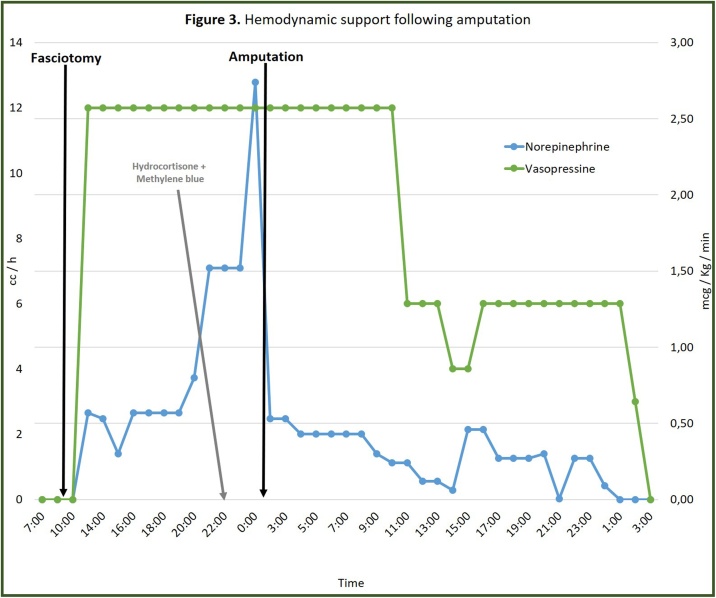
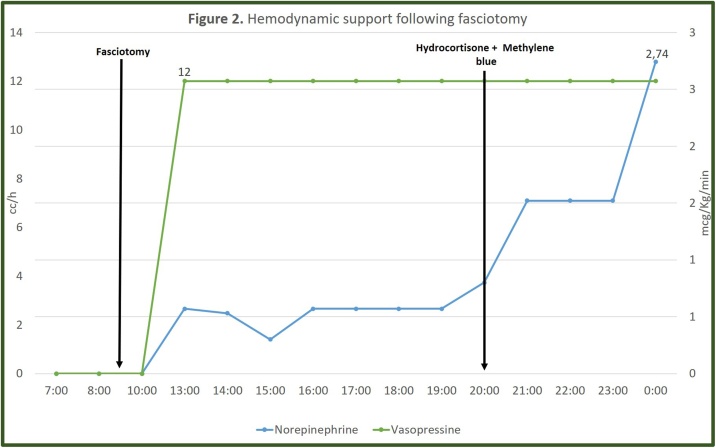
This is a 29-year-old patient whose lower body was trapped for 50 h under a 40-meter landslide. Upon admission the left thigh was edematous and painful. Laboratories revealed a creatinine of 1.58 mg/dL, hyperkalemia, metabolic acidosis, hyperlactatemia and creatinine phosphokinase (CPK) of 88,700 U/L, suggesting CS. Despite fluid and bicarbonate infusion his renal function worsened, CPK rose and left thigh became more tense, so a fasciotomy was performed. He developed a distributive shock refractory to vasopressors, steroids and methylene blue so amputation was proposed. Two hours after amputation the vasopressor support was nearly withdrawn.
This case suggests a potential benefit of amputation in patients with CS and progressive deterioration despite aggressive resuscitation. It also invites to think if this is a decision that should be considered before the establishment or in the initial stages of the syndrome, even if the viability of the extremity is still questionable.
The presence of risk factors for poor prognosis can favor amputation despite the apparent viability of the limb and the morbidity of losing an extremity.
挤压综合征(CS)是一种继发于严重横纹肌溶解和再灌注损伤,因严重电解质紊乱、循环功能障碍及多器官功能衰竭而导致高发病率和死亡率的病症。对于筋膜切开术在挤压伤所致骨筋膜室综合征治疗中的作用存在争议,早期截肢是否对患者有益仍不明确。
本病例为一名29岁患者,其下半身被埋在40米的山体滑坡下达50小时。入院时左大腿肿胀且疼痛。实验室检查显示肌酐为1.58mg/dL、高钾血症、代谢性酸中毒、高乳酸血症以及肌酸磷酸激酶(CPK)为88,700U/L,提示为挤压综合征。尽管输注了液体和碳酸氢盐,其肾功能仍恶化,CPK升高,左大腿变得更加紧张,因此进行了筋膜切开术。他出现了对血管升压药、类固醇和亚甲蓝均无效的分布性休克,于是建议进行截肢。截肢两小时后,血管升压药支持基本撤除。
该病例提示对于挤压综合征患者,尽管积极复苏但病情仍进行性恶化时,截肢可能有益。这也引发思考,即使肢体的存活能力仍有疑问,这是否是在综合征确立前或初始阶段就应考虑的决定。
尽管肢体表面仍有存活能力且截肢存在致残风险,但存在预后不良的危险因素时仍可能有利于截肢。