Division of Infectious Diseases and International Health, Duke University School of Medicine, Durham, North Carolina, USA.
Oxford University Clinical Research Unit, Ho Chi Minh City, Vietnam.
Clin Infect Dis. 2021 Jul 15;73(2):e330-e336. doi: 10.1093/cid/ciaa826.
Talaromycosis is an invasive mycosis endemic in Southeast Asia and causes substantial morbidity and mortality in individuals with advanced human immunodeficiency virus (HIV) disease. Current diagnosis relies on isolating Talaromyces marneffei in cultures, which takes up to 14 days and is detectable only during late-stage infection, leading to high mortality.
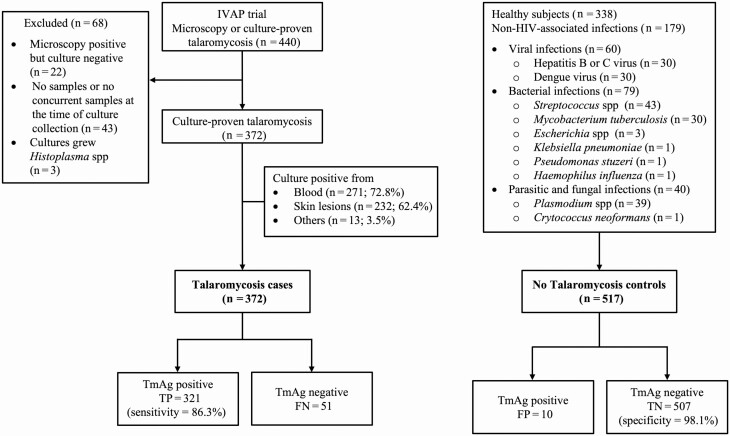
In this retrospective case-control study, we assessed the accuracy of a novel Mp1p antigen-detecting enzyme immunoassay (EIA) in stored plasma samples of 372 patients who had culture-proven talaromycosis from blood or sterile body fluids (reference standard) and 517 individuals without talaromycosis (338 healthy volunteers; 179 with other infections). All participants were recruited between 2011 and 2017 in Vietnam.
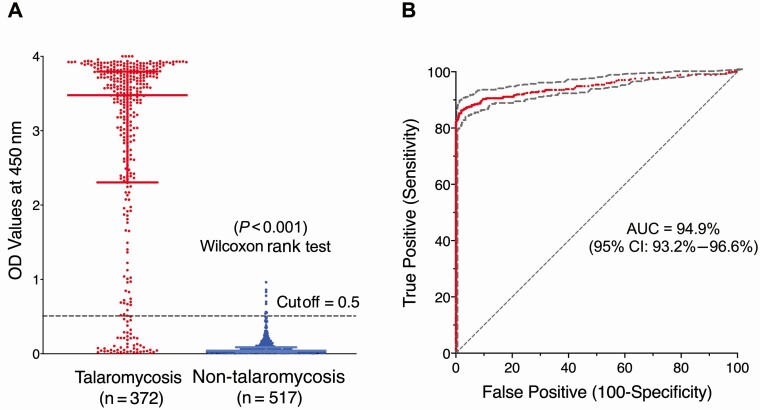
Of cases and controls, 66.1% and 75.4%, respectively, were male; the median age was 33 and 37, respectively. All cases were HIV infected; median CD4 count was 10 cells/μL. At an optical density cutoff of 0.5, the specificity was 98.1% (95% CI, 96.3%-99.0%); the sensitivity was superior to blood culture (86.3% [95% CI, 82.3%-89.5%] vs 72.8% [95% CI, 68.0%-77.2%]) (P < .001, McNemar test). The time to diagnosis was 6 hours vs 6.6 ± 3.0 days for blood culture. Paired plasma and urine testing in the same patients (n = 269) significantly increased sensitivity compared to testing plasma alone or testing urine alone (P < .001 and P = .02, respectively, McNemar test).
The Mp1p EIA is highly specific and is superior in sensitivity and time to diagnosis compared to blood culture for the diagnosis of talaromycosis. Paired plasma and urine testing further increases sensitivity, introducing a new tool for rapid diagnosis, enabling early treatment and potentially reducing mortality.
足放线菌病是一种侵袭性真菌感染,流行于东南亚地区,在人类免疫缺陷病毒(HIV)感染晚期患者中发病率和死亡率较高。目前的诊断依赖于在培养物中分离马尔尼菲篮状菌,这需要长达 14 天的时间,并且只能在感染晚期检测到,导致死亡率较高。
在这项回顾性病例对照研究中,我们评估了一种新型 Mp1p 抗原检测酶免疫分析(EIA)在 372 例经血液或无菌体液培养证实的马尔尼菲篮状菌感染患者(参考标准)和 517 例无马尔尼菲篮状菌感染患者(338 例健康志愿者;179 例其他感染患者)的储存血浆样本中的准确性。所有参与者均于 2011 年至 2017 年在越南招募。
病例组和对照组中,分别有 66.1%和 75.4%为男性;中位年龄分别为 33 岁和 37 岁。所有病例均为 HIV 感染;中位 CD4 计数为 10 个/μL。在光密度截止值为 0.5 时,特异性为 98.1%(95%置信区间,96.3%-99.0%);敏感性优于血培养(86.3%[95%置信区间,82.3%-89.5%] vs 72.8%[95%置信区间,68.0%-77.2%])(P <.001,McNemar 检验)。与血培养相比,诊断时间为 6 小时 vs 6.6 ± 3.0 天。对同一名患者的配对血浆和尿液检测(n = 269)与仅检测血浆或仅检测尿液相比,显著提高了敏感性(P <.001 和 P =.02,McNemar 检验)。
与血培养相比,Mp1p EIA 具有高度特异性,在敏感性和诊断时间方面均优于血培养,可用于诊断马尔尼菲篮状菌病。血浆和尿液配对检测进一步提高了敏感性,为快速诊断引入了一种新工具,可实现早期治疗,降低死亡率。