Doctor of Public Health Program, Harvard T.H. Chan School of Public Health, Boston, Massachusetts, United States of America.
Division of Infectious Diseases, Massachusetts General Hospital, Boston, Massachusetts, United States of America.
PLoS Negl Trop Dis. 2020 Jun 22;14(6):e0008398. doi: 10.1371/journal.pntd.0008398. eCollection 2020 Jun.
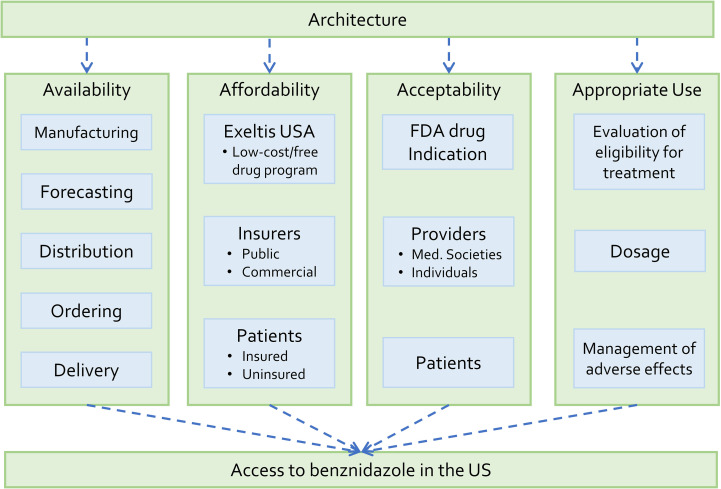
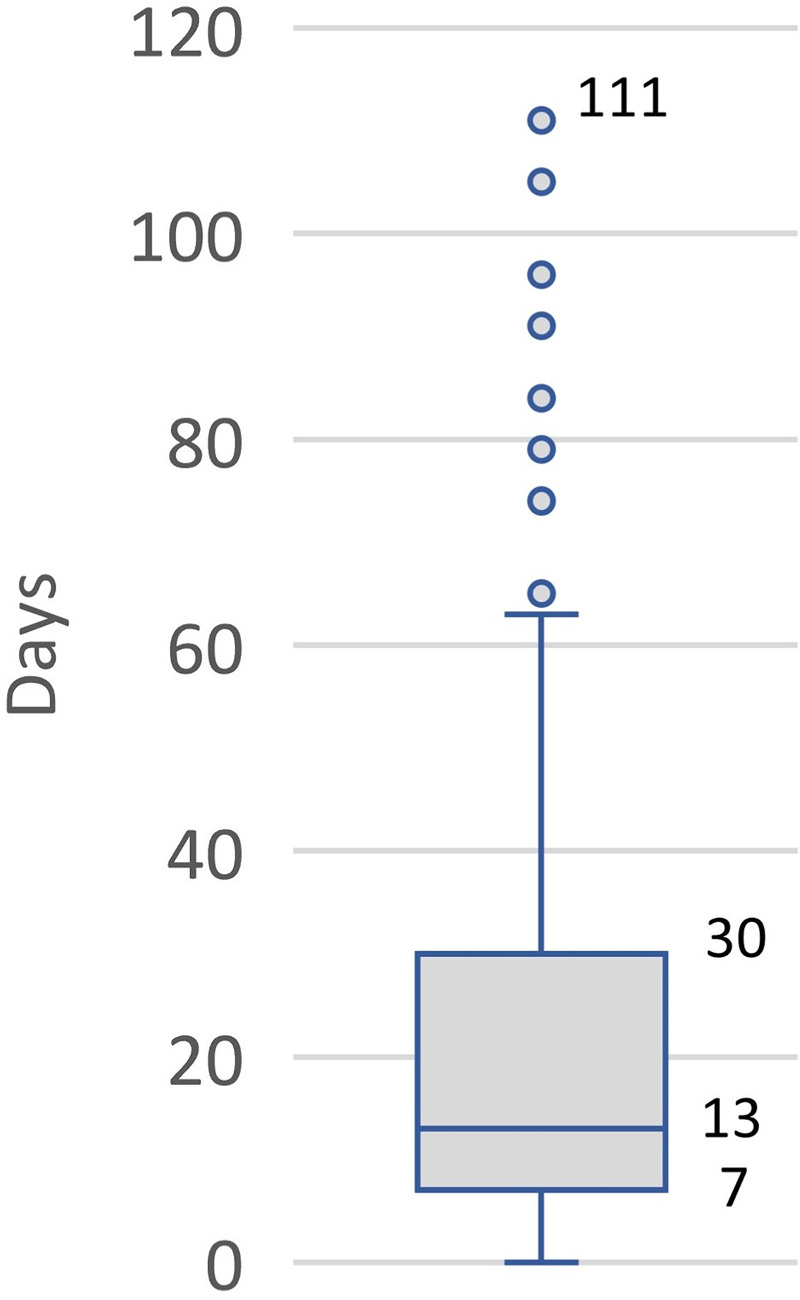
Approximately 300,000 persons in the United States (US) are infected with Trypanosoma cruzi, the protozoan that causes Chagas disease, but less than 1% are estimated to have received antiparasitic treatment. Benznidazole was approved by the US Food and Drug Administration (FDA) for treatment of T. cruzi infection in 2017 and commercialized in May 2018. This paper analyzes factors that affect access to benznidazole following commercialization and suggests directions for future actions to expand access. We applied an access framework to identify barriers, facilitators, and key actors that influence the ability of people with Chagas disease to receive appropriate treatment with benznidazole. Data were collected from the published literature, key informants, and commercial databases. We found that the mean number of persons who obtained benznidazole increased from just under 5 when distributed by the CDC to 13 per month after the commercial launch (from May 2018 to February 2019). Nine key barriers to access were identified: lack of multi-sector coordination, failure of health care providers to use a specific order form, lack of an emergency delivery system, high medical costs for uninsured patients, narrow indications for use of benznidazole, lack of treatment guidelines, limited number of qualified treaters, difficulties for patients to make medical appointments, and inadequate evaluation by providers to determine eligibility for treatment. Our analysis shows that access to benznidazole is still limited after FDA approval. We suggest six areas for strategic action for the pharmaceutical company that markets benznidazole and its allied private foundation to expand access to benznidazole in the US. In addition, we recommend expanding the existing researcher-clinician network by including government agencies, companies and others. This paper's approach could be applied to access programs for benznidazole in other countries or for other health products that target neglected populations throughout the world.
美国约有 30 万人感染克氏锥虫,这种原生动物会导致恰加斯病,但据估计,只有不到 1%的人接受了驱虫治疗。贝那唑嗪于 2017 年获得美国食品和药物管理局(FDA)批准用于治疗克氏锥虫感染,并于 2018 年 5 月商业化。本文分析了商业化后获得贝那唑嗪的影响因素,并提出了扩大获得途径的未来行动方向。我们应用获取框架来确定影响恰加斯病患者获得适当贝那唑嗪治疗能力的障碍、促进因素和关键行为者。数据来自已发表的文献、主要信息来源和商业数据库。我们发现,自 2018 年 5 月(商业化启动后)以来,获得贝那唑嗪的人数从 CDC 分发时的略低于 5 人增加到每月 13 人。确定了 9 个获取障碍:缺乏多部门协调、医疗保健提供者未能使用特定订单表、缺乏紧急交付系统、未参保患者的医疗费用高、贝那唑嗪使用适应症狭窄、缺乏治疗指南、合格治疗者数量有限、患者预约困难以及提供者评估不足以确定治疗资格。我们的分析表明,FDA 批准后,贝那唑嗪的可及性仍然有限。我们建议为营销贝那唑嗪及其相关私人基金会的制药公司提出六个战略行动领域,以扩大贝那唑嗪在美国的可及性。此外,我们建议通过包括政府机构、公司和其他机构来扩大现有的研究人员-临床医生网络。本文的方法可应用于其他国家或针对全世界被忽视人群的其他卫生产品的贝那唑嗪获取方案。