Martinez-Pérez Angela, Soriano-Pérez Manuel Jesús, Salvador Fernando, Gomez-Junyent Joan, Villar-Garcia Judith, Santin Miguel, Muñoz Carme, González-Cordón Ana, Salas-Coronas Joaquín, Sulleiro Elena, Somoza Dolors, Treviño Begoña, Pecorelli Rosángela, Llaberia-Marcual Jaume, Lozano-Serrano Ana Belén, Quinto Llorenç, Muñoz Jose, Requena-Méndez Ana, Strong-Semtsi Working Group On Behalf Of The
CAP Casanova, Consorci d'Atenció Primaria en Salut Barcelona Esquerra, 08036 Barcelona, Spain.
Barcelona Institute for Global Health, ISGlobal-Hospital Clinic, Universitat de Barcelona, 08036 Barcelona, Spain.
Pathogens. 2020 Jun 23;9(6):507. doi: 10.3390/pathogens9060507.
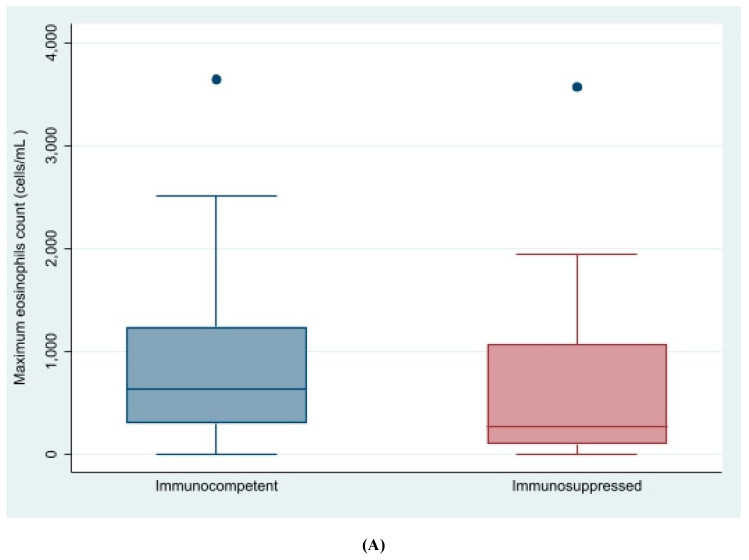
is a widely distributed nematode more frequent in tropical areas and particularly severe in immunosuppressed patients. The aim of this study was to determine factors associated with strongyloidiasis in migrants living in a non-endemic area and to assess the response to treatment and follow-up in those diagnosed with the infection. We performed a multicenter case-control study with 158 cases and 294 controls matched 1:2 by a department service. Participants were recruited simultaneously at six hospitals or clinics in Spain. A paired-match analysis was then performed looking for associations and odds ratios in sociodemographic characteristics, pathological background, clinical presentation and analytical details. Cases outcomes after a six-month follow-up visit were also registered and their particularities described. Most cases and controls came from Latin America (63%-47%) or sub-Saharan Africa (26%-35%). The number of years residing in Spain (9.9 vs. 9.8, = 0.9) and immunosuppression status (30% vs. 36.3%, = 0.2) were also similar in both groups. Clinical symptoms such as diffuse abdominal pain (21% vs. 13%, = 0.02), and epigastralgia (29% vs. 18%, < 0.001); along with a higher eosinophil count (483 vs. 224 cells/mL in cases and controls, < 0.001) and the mean total Immunoglobulin E (IgE) (354 U/L vs. 157.9 U/L; < 0.001) were associated with having strongyloidiasis. Finally, 98.2% percent of the cases were treated with ivermectin in different schedules, and 94.5% met the cure criteria at least six months after their first consultation. Abdominal pain, epigastralgia, eosinophilia, increased levels of IgE and Latin American origin remain the main features associated with infection, although this association is less evident in immunosuppressed patients. The appropriate follow-up time to evaluate treatment response based on serology titers should be extended beyond 6 months if the cure criteria are not achieved.
是一种广泛分布的线虫,在热带地区更为常见,在免疫抑制患者中尤为严重。本研究的目的是确定生活在非流行地区的移民中与类圆线虫病相关的因素,并评估确诊感染患者的治疗反应和随访情况。我们进行了一项多中心病例对照研究,有158例病例和294例对照,按科室服务1:2匹配。参与者在西班牙的六家医院或诊所同时招募。然后进行配对匹配分析,寻找社会人口学特征、病理背景、临床表现和分析细节中的关联和比值比。还记录了六个月随访后的病例结果并描述了其特殊性。大多数病例和对照来自拉丁美洲(63%-47%)或撒哈拉以南非洲(26%-35%)。两组在西班牙居住的年数(9.9对9.8,P = 0.9)和免疫抑制状态(30%对36.3%,P = 0.2)也相似。临床症状如弥漫性腹痛(21%对13%,P = 0.02)和上腹部疼痛(29%对18%,P < 0.001);以及较高的嗜酸性粒细胞计数(病例组和对照组分别为483对224个细胞/毫升,P < 0.001)和平均总免疫球蛋白E(IgE)(354 U/L对157.9 U/L;P < 0.001)与类圆线虫病有关。最后,98.2%的病例接受了不同疗程的伊维菌素治疗,94.5%在首次咨询后至少六个月达到治愈标准。腹痛、上腹部疼痛、嗜酸性粒细胞增多、IgE水平升高和拉丁美洲血统仍然是与感染相关的主要特征,尽管这种关联在免疫抑制患者中不太明显。如果未达到治愈标准,基于血清学滴度评估治疗反应的适当随访时间应延长至6个月以上。