Memorial Sloan-Kettering Cancer Center, New York, New York.
The Angeles Clinic and Research Institute, Los Angeles, California.
Clin Cancer Res. 2020 Sep 1;26(17):4531-4541. doi: 10.1158/1078-0432.CCR-20-0328. Epub 2020 Jun 25.
The study goal was to determine safety, antitumor activity, and pharmacodynamic profile of mogamulizumab, an anti-C-C chemokine receptor 4 (anti-CCR4) mAb targeting effector regulatory T cells (eTreg), in combination with mAb checkpoint inhibitors durvalumab or tremelimumab.
This was a multicenter, phase I, dose escalation study, followed by disease-specific cohort expansion (NCT02301130). Mogamulizumab dose escalation proceeded with concurrent dose escalation of durvalumab or tremelimumab in patients with advanced solid tumors. Cohort expansion occurred with mogamulizumab 1 mg/kg plus durvalumab 10 mg/kg or tremelimumab 10 mg/kg in patients with advanced pancreatic cancer.
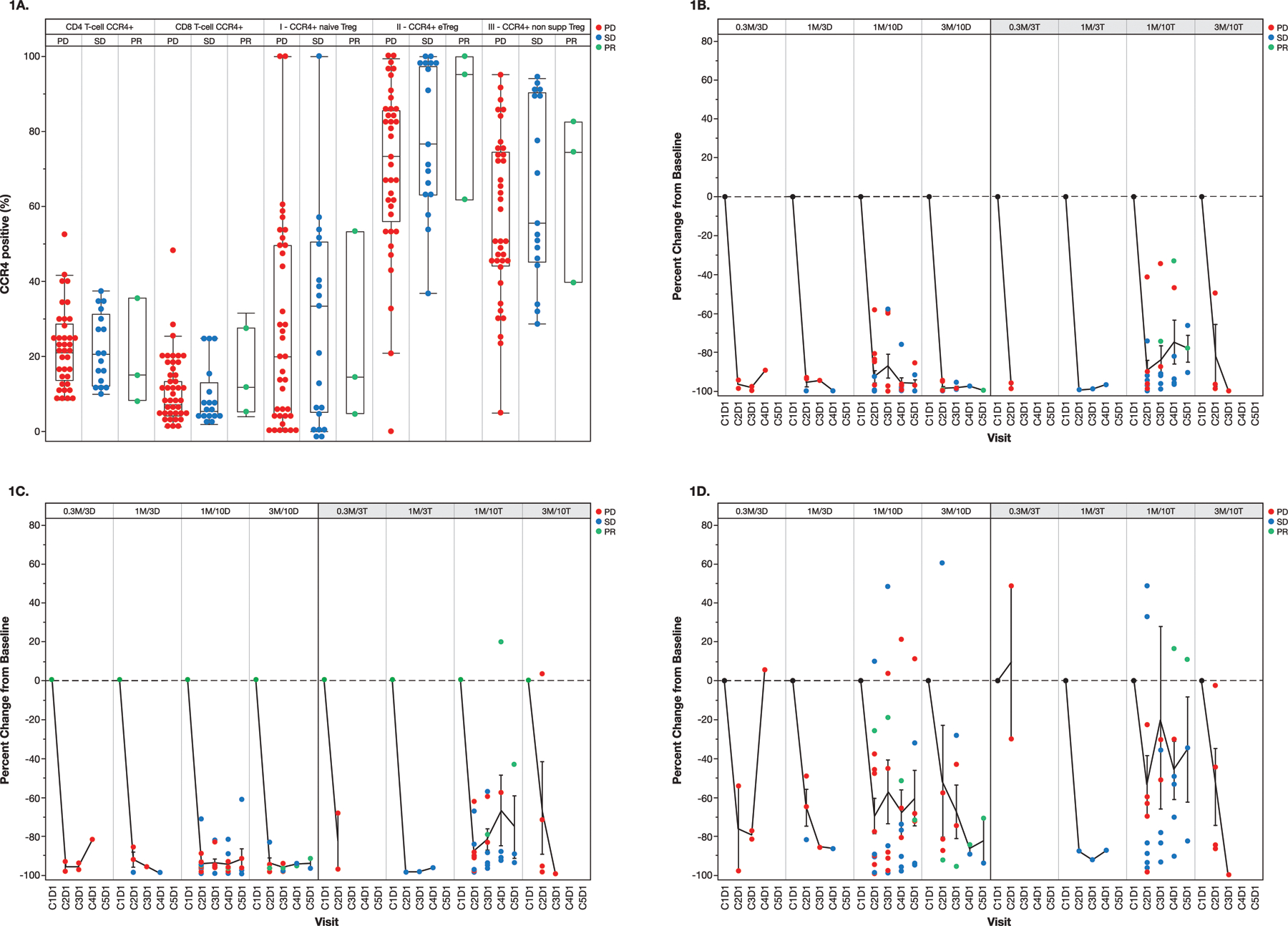
Forty patients were enrolled during dose escalation, followed by 24 patients during dose expansion. No dose-limiting toxicities occurred during dose escalation. No new or unexpected toxicities were seen. Tolerability, the primary endpoint, was acceptable utilizing mogamulizumab 1 mg/kg plus durvalumab or tremelimumab 10 mg/kg in the combined dose escalation and dose expansion cohorts (each = 19). At these doses, the objective response rate was 5.3% (95% confidence interval, 0.1%-26.0%; one partial response) with each combination treatment. At all doses, mogamulizumab treatment led to almost complete depletion of peripheral eTregs, as well as reduction of intratumoral Tregs in the majority of patients. There was no clear correlation of clinical response with peripheral or intratumoral reduction in CCR4 eTregs or with baseline degree of CCR4 expression.
Mogamulizumab in combination with durvalumab or tremelimumab did not result in potent antitumor efficacy in patients with advanced solid tumors. Tolerability of mogamulizumab 1 mg/kg combined with durvalumab or tremelimumab 10 mg/kg was acceptable.
本研究旨在评估莫格利珠单抗(一种针对效应调节性 T 细胞(eTreg)的抗 C-C 趋化因子受体 4(抗 CCR4)单克隆抗体)联合 mAb 检查点抑制剂度伐鲁单抗或替西木单抗的安全性、抗肿瘤活性和药效学特征。
这是一项多中心、I 期、剂量递增研究,随后进行了疾病特异性队列扩展(NCT02301130)。在晚期实体瘤患者中,莫格利珠单抗剂量递增的同时进行度伐鲁单抗或替西木单抗的剂量递增。在晚期胰腺癌患者中,进行了莫格利珠单抗 1 mg/kg 联合度伐鲁单抗 10 mg/kg 或替西木单抗 10 mg/kg 的队列扩展。
在剂量递增期间,共招募了 40 例患者,随后在剂量扩展期间,共招募了 24 例患者。在剂量递增期间未发生剂量限制毒性。未观察到新的或意外的毒性。在联合剂量递增和剂量扩展队列中,莫格利珠单抗 1 mg/kg 联合度伐鲁单抗或替西木单抗 10 mg/kg 的耐受性是可接受的,主要终点(n=19)。在这些剂量下,两种联合治疗的客观缓解率均为 5.3%(95%置信区间,0.1%-26.0%;1 例部分缓解)。在所有剂量下,莫格利珠单抗治疗导致外周 eTreg 几乎完全耗尽,并且大多数患者的肿瘤内 Treg 减少。临床反应与外周或肿瘤内 CCR4 eTreg 减少或 CCR4 表达的基线程度之间没有明确的相关性。
莫格利珠单抗联合度伐鲁单抗或替西木单抗在晚期实体瘤患者中未产生显著的抗肿瘤疗效。莫格利珠单抗 1 mg/kg 联合度伐鲁单抗或替西木单抗 10 mg/kg 的耐受性可接受。