Division of Diabetes, Endocrinology and Clinical Immunology, Department of Internal Medicine, Hyogo College of Medicine, Nishinomiya, Japan.
Azuma Diabetes Clinic, Nishinomiya, Hyogo, Japan.
J Diabetes Investig. 2021 Feb;12(2):244-253. doi: 10.1111/jdi.13336. Epub 2020 Aug 2.
AIMS/INTRODUCTION: Continuous glucose monitoring (CGM) metrics, such as times in range (TIR) and time below range, have been shown to be useful as clinical targets that complement glycated hemoglobin (HbA1c) for patients with type 2 diabetes mellitus. We investigated the relationships between TIR, glycemic variability and patient characteristics in patients with type 2 diabetes mellitus.
We carried out continuous glucose monitoring in 281 outpatients with type 2 diabetes mellitus who participated in a multicenter cohort (Hyogo Diabetes Hypoglycemia Cognition Complications) study.
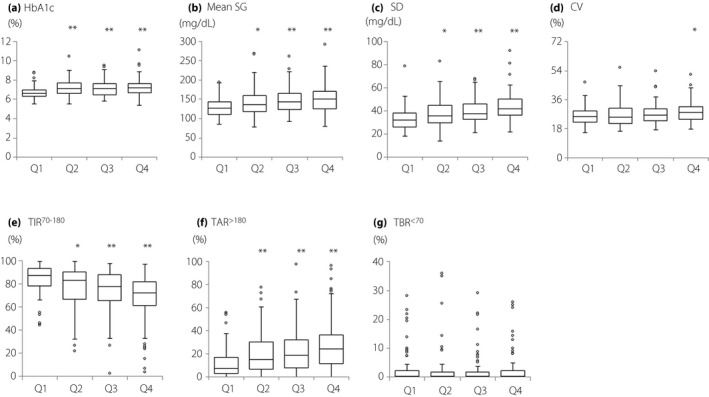
The results are shown as the median (interquartile range). The age, disease duration and HbA1c were 68 years (62-71 years), 13 years (7-23 years) and 6.9% (6.5-7.5%), respectively. TIR and standard deviation obtained by continuous glucose monitoring worsened significantly with increasing disease duration. Multiple regression analyses showed that disease duration (standard partial regression coefficient, β = -0.160, P = 0.003), diabetic peripheral neuropathy (β = -0.106, P = 0.033) and urinary albumin excretion (β = -0.100, P = 0.043) were useful explanatory factors for TIR. In contrast, HbA1c (β = -0.398, P < 0.001) and the use of antidiabetic drugs potentially associated with severe hypoglycemia (β = 0.180, P = 0.028), such as sulfonylureas, glinides and insulin, were useful explanatory factors for time below range in the elderly patients with type 2 diabetes mellitus.
The results of this study suggest that disease duration and diabetic complications are associated with TIR deterioration. In addition, low HbA1c levels and the use of antidiabetic drugs potentially associated with severe hypoglycemia might worsen the time below range in the elderly.
目的/引言:连续血糖监测(CGM)的各项指标,如血糖控制在目标范围内时间(TIR)和血糖低于目标范围时间,已被证明对于 2 型糖尿病患者是有用的临床目标,可以补充糖化血红蛋白(HbA1c)。我们研究了 281 例 2 型糖尿病患者的 TIR、血糖变异性与患者特征之间的关系。
我们对参加多中心队列(兵库糖尿病低血糖认知并发症)研究的 281 例 2 型糖尿病门诊患者进行了连续血糖监测。
结果以中位数(四分位距)表示。患者的年龄、病程和 HbA1c 分别为 68 岁(62-71 岁)、13 年(7-23 年)和 6.9%(6.5-7.5%)。随着病程的延长,CGM 获得的 TIR 和标准差显著恶化。多元回归分析显示,病程(标准偏回归系数,β=-0.160,P=0.003)、糖尿病周围神经病变(β=-0.106,P=0.033)和尿白蛋白排泄(β=-0.100,P=0.043)是 TIR 的有用解释因素。相反,HbA1c(β=-0.398,P<0.001)和可能与严重低血糖相关的降糖药物(β=0.180,P=0.028),如磺脲类、格列奈类和胰岛素,是老年 2 型糖尿病患者血糖低于目标范围的有用解释因素。
本研究结果表明,病程和糖尿病并发症与 TIR 恶化有关。此外,较低的 HbA1c 水平和可能与严重低血糖相关的降糖药物的使用可能会使老年患者血糖低于目标范围的时间恶化。