Braun Barbara I, Chitavi Salome O, Perkins Kiran M, Perz Joseph F, Link-Gelles Ruth, Hoppe Jennifer, Donofrio Kristine M, Shen Yanhong, Garcia-Houchins Sylvia
Jt Comm J Qual Patient Saf. 2020 Sep;46(9):531-541. doi: 10.1016/j.jcjq.2020.05.005. Epub 2020 May 23.
Beginning in October 2016, the Centers for Medicare & Medicaid Services (CMS) issued expanded guidance requiring accrediting organizations and state survey agencies to report serious infection control breaches to relevant state health departments. This project sought to characterize and summarize The Joint Commission's early experiences and findings in applying this guidance to facilities accredited under the ambulatory and office-based surgery programs in 2017.
Surveyor notes were retrospectively reviewed to identify individual breaches, and then the Centers for Disease Control and Prevention's Infection Prevention Checklist for Outpatient Settings was used to categorize and code documented breaches.
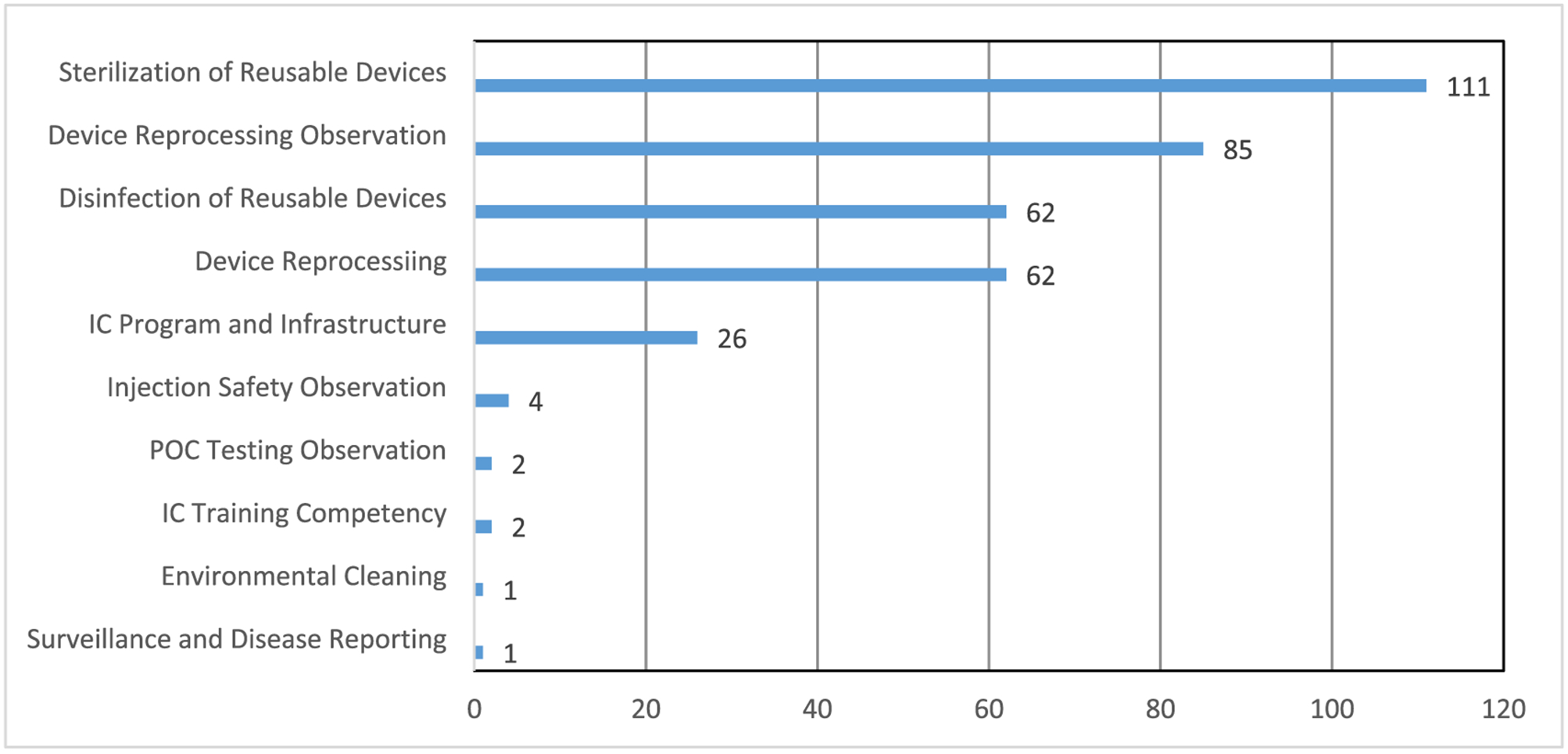
Of 845 ambulatory organizations, 39 (4.6%) had breaches observed during the survey process and reported to health departments. Within these organizations, surveyors documented 356 breaches, representing 52 different breach codes. Common breach domains were sterilization of reusable devices, device reprocessing observation, device reprocessing, disinfection of reusable devices, and infection control program and infrastructure. Eight of the 39 facilities (20.5%) were cited for not performing the minimum level of reprocessing based on the items' intended use, reusing single-use devices, and/or not using aseptic technique to prepare injections.
The CMS infection control breach reporting requirement has helped highlight some of the challenges faced by ambulatory facilities in providing a safe care environment for their patients. This analysis identified numerous opportunities for improved staff training and competencies as well as leadership oversight and investment in necessary resources. More systematic assessments of infection control practices, extending to both accredited and nonaccredited ambulatory facilities, are needed to inform oversight and prevention efforts.
从2016年10月开始,医疗保险和医疗补助服务中心(CMS)发布了扩展指南,要求认证组织和州调查机构向相关州卫生部门报告严重的感染控制违规行为。本项目旨在描述和总结联合委员会在2017年将该指南应用于门诊和门诊手术项目认证设施时的早期经验和发现。
对调查员记录进行回顾性审查以识别个体违规行为,然后使用疾病控制与预防中心的门诊环境感染预防检查表对记录的违规行为进行分类和编码。
在845个门诊机构中,有39个(4.6%)在调查过程中出现违规行为并报告给了卫生部门。在这些机构中,调查员记录了356起违规行为,代表52种不同的违规代码。常见的违规领域包括可重复使用设备的灭菌、设备再处理观察、设备再处理、可重复使用设备的消毒以及感染控制计划和基础设施。39个设施中有8个(20.5%)因未根据物品预期用途进行最低水平的再处理、重复使用一次性设备和/或未使用无菌技术准备注射而被引用。
CMS的感染控制违规报告要求有助于突出门诊设施在为患者提供安全护理环境方面面临的一些挑战。该分析确定了许多改进员工培训和能力以及领导力监督和对必要资源投资的机会。需要对感染控制实践进行更系统的评估,包括认证和未认证的门诊设施,以为监督和预防工作提供信息。