Lappas Martha, Lim Ratana, Price Sarah, Prendergast Luke A, Proietto Joseph, Ekinci Elif I, Sumithran Priya
University of Melbourne, Department of Obstetrics and Gynaecology, Melbourne, Australia.
Mercy Hospital for Women, Melbourne, Australia.
Int J Womens Health. 2020 Jun 15;12:455-462. doi: 10.2147/IJWH.S241785. eCollection 2020.
Central homeostatic regulation of fat stores is attenuated during pregnancy, to allow for adequate fat deposition to support fetal development and lactation. What factors particular to pregnancy facilitate fat accumulation, and why gestational weight gain (GWG) is so variable, are not clear. The aim of this cross-sectional study was to examine the associations between GWG and circulating hormones with known effects on appetite and growth.
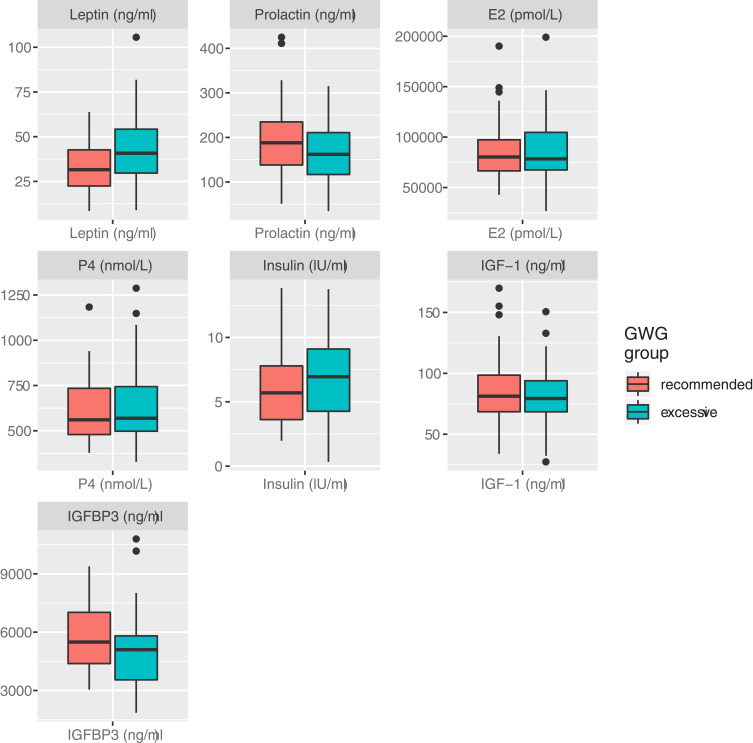
Women without obesity (body mass index, BMI <30 kg/m), with a healthy singleton pregnancy, were recruited at the time of delivery by elective Caesarean section at a tertiary obstetric hospital. Women with preterm (<37 weeks) delivery and smokers were excluded. Maternal blood was collected at the time of delivery for measurement of fasting oestradiol, progesterone, prolactin, insulin, leptin, insulin-like growth factor 1 and insulin-like growth factor binding protein 3. Comparisons were made between women who gained weight within the range recommended by Institute of Medicine guidelines for normal weight women (11.5-16 kg; n=34) and those who gained excessive weight (>16 kg; n=35) during pregnancy. Analysis of covariance was carried out using multiple linear regression to test the effect of GWG group on biochemical parameters, accounting for pre-pregnancy BMI.
The 69 participants had a mean age of 34.6 ± 4.3 years, and pre-pregnancy BMI of (23.3 ± 1.8 kg/m), with no significant differences between groups in pre-pregnancy weight, BMI, age, birthweight or parity. Mean GWG was 14.0 ± 1.3 kg in the "recommended" group and 19.6 ± 3.2 kg in the "excessive" group. Leptin was significantly higher (43.4 ± 21.6 vs 33.4 ± 15.0 ng/mL, p=0.03) and prolactin tended to be lower (159.5 ± 66.1 vs 194.0 ± 85.6 ng/mL, p=0.07) at delivery in women with excessive (vs recommended) GWG. No other circulating factors were found to differ between groups. The between-group difference in leptin remained after adjustment for pre-pregnancy BMI in multiple linear regression and quantile regression analyses.
In women without obesity, leptin remains a marker of adiposity during pregnancy. GWG was not associated with other circulating hormones with effects on appetite and growth.
孕期脂肪储备的中枢稳态调节功能减弱,以便有足够的脂肪沉积来支持胎儿发育和哺乳。孕期特有的哪些因素促进了脂肪积累,以及为什么孕期体重增加(GWG)如此多变,目前尚不清楚。这项横断面研究的目的是探讨GWG与已知对食欲和生长有影响的循环激素之间的关联。
在一家三级产科医院,通过择期剖宫产在分娩时招募无肥胖(体重指数,BMI<30kg/m²)、单胎健康妊娠的女性。排除早产(<37周)和吸烟的女性。在分娩时采集母体血液,用于测量空腹雌二醇、孕酮、催乳素、胰岛素、瘦素、胰岛素样生长因子1和胰岛素样生长因子结合蛋白3。对体重增加在医学研究所指南推荐的正常体重女性范围内(11.5-16kg;n=34)和孕期体重增加过多(>16kg;n=35)的女性进行比较。使用多元线性回归进行协方差分析,以检验GWG组对生化参数的影响,并考虑孕前BMI。
69名参与者的平均年龄为34.6±4.3岁,孕前BMI为(23.3±1.8kg/m²),两组在孕前体重、BMI、年龄、出生体重或产次方面无显著差异。“推荐”组的平均GWG为14.0±1.3kg,“过多”组为19.6±3.2kg。GWG过多(与推荐相比)的女性在分娩时瘦素显著更高(43.4±21.6对33.4±15.0ng/mL,p=0.03),催乳素倾向于更低(159.5±66.1对194.0±85.6ng/mL,p=0.07)。未发现其他循环因子在两组之间存在差异。在多元线性回归和分位数回归分析中,调整孕前BMI后,两组之间瘦素的差异仍然存在。
在无肥胖的女性中,瘦素仍然是孕期肥胖的一个标志物。GWG与其他对食欲和生长有影响的循环激素无关。