Department of Trauma and Orthopaedic Surgery, University Medical Center Hamburg-Eppendorf, Hamburg, Germany.
Eur J Trauma Emerg Surg. 2020 Dec;46(6):1211-1219. doi: 10.1007/s00068-020-01422-0. Epub 2020 Jun 30.
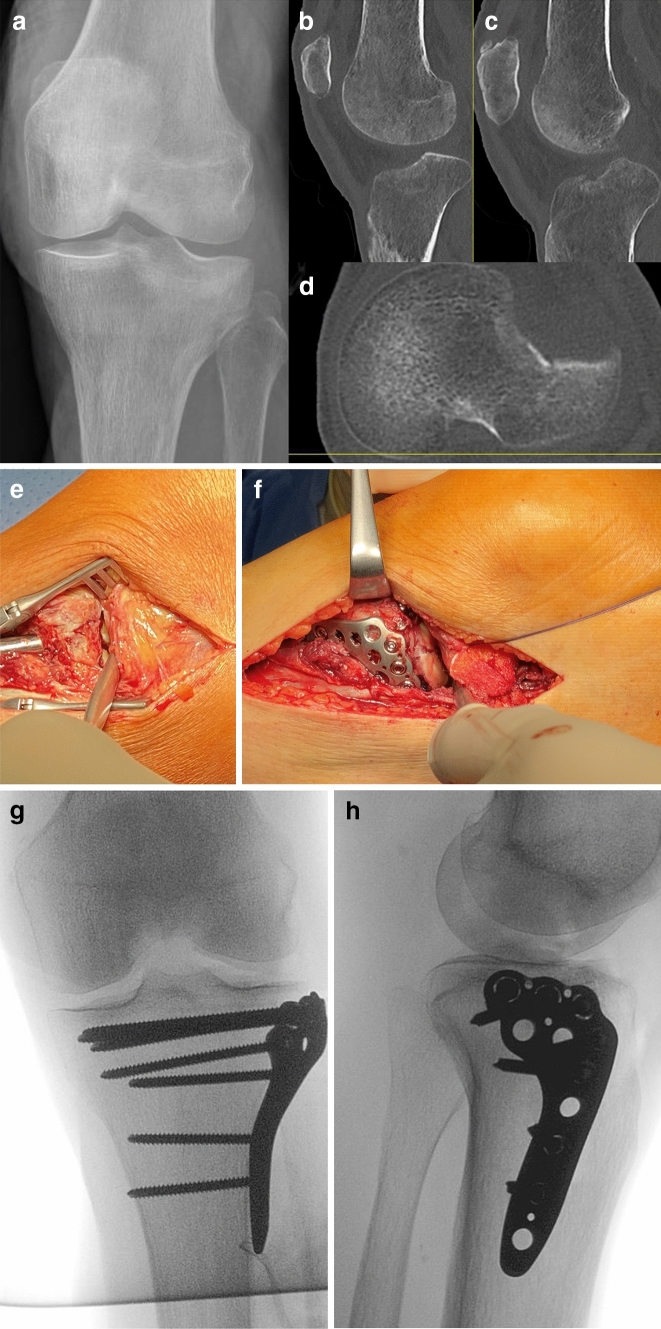
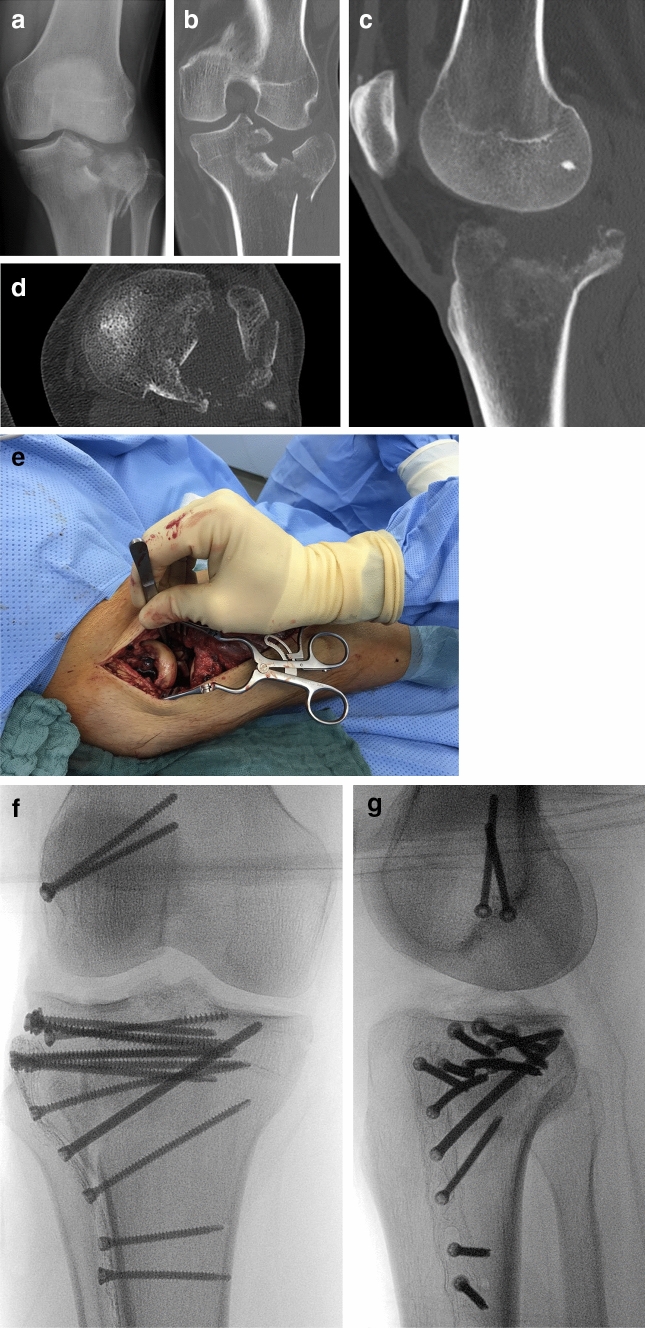
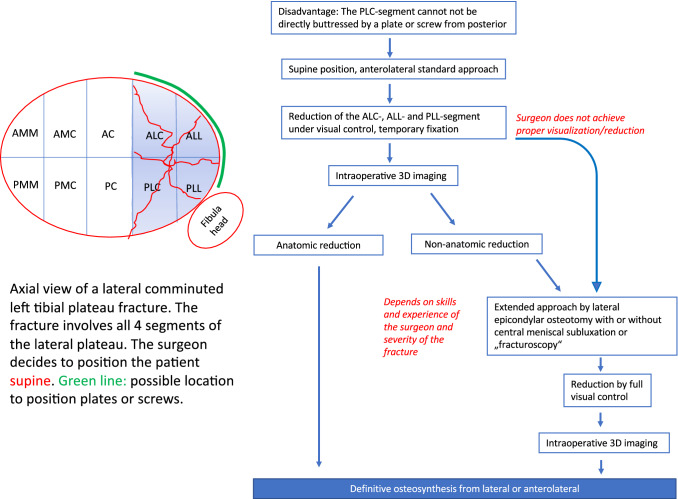
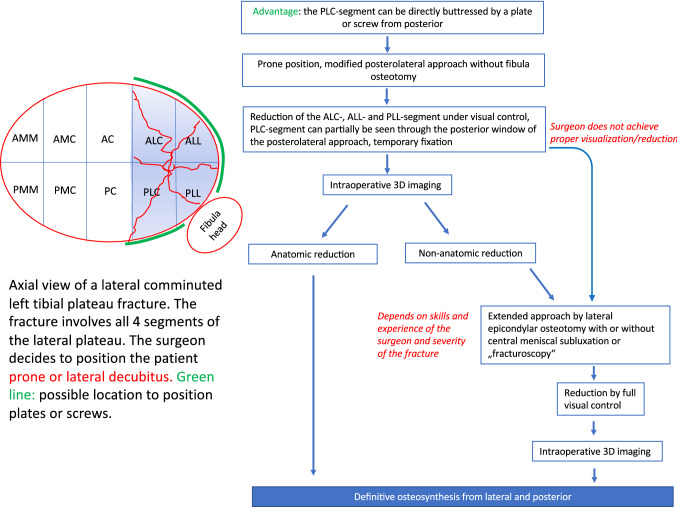
Malreduction after tibial plateau fractures mainly occurs due to insufficient visualization of the articular surface. In 85% of all C-type fractures an involvement of the posterolateral-central segment is observed, which is the main region of malreduction. The choice of the approach is determined (1) by the articular area which needs to be visualized and (2) the positioning of the fixation material. For simple lateral plateau fractures without involvement of the posterolateral-central segment an anterolateral standard approach in supine position with a lateral plating is the treatment of choice in most cases. For complex fractures the surgeon has to consider, that the articular surface of the lateral plateau only can be completely visualized by extended approaches in supine, lateral and prone position. Anterolateral and lateral plating can also be performed in supine, lateral and prone position. A direct fixation of the posterolateral-central segment by a plate or a screw from posterior can be only achieved in prone or lateral position, not supine. The posterolateral approach includes the use of two windows for direct visualization of the fracture. If visualization is insufficient the approach can be extended by lateral epicondylar osteotomy which allows exposure of at least 83% of the lateral articular surface. Additional central subluxation of the lateral meniscus allows to expose almost 100% of the articular surface. The concept of stepwise extension of the approach is helpful and should be individually performed as needed to achieve anatomic reduction and stable fixation of tibial plateau fractures.
胫骨平台骨折后复位不良主要是由于关节面显示不足所致。在所有 C 型骨折中,85%观察到后外侧-中央段受累,这是复位不良的主要部位。入路的选择取决于需要可视化的关节区域和(2)固定材料的定位。对于单纯外侧平台骨折,无后外侧-中央段受累,大多数情况下,仰卧位前外侧标准入路加外侧钢板固定是首选治疗方法。对于复杂骨折,外科医生必须考虑到外侧平台的关节面只有通过仰卧位、侧卧位和俯卧位的扩展入路才能完全可视化。仰卧位、侧卧位和俯卧位也可以进行前外侧和外侧钢板固定。通过从后方的钢板或螺钉直接固定后外侧-中央段只能在俯卧位或侧卧位进行,而不能在仰卧位进行。后外侧入路包括使用两个窗口直接观察骨折。如果显示不足,可以通过外侧髁突切开术扩展入路,这可以暴露至少 83%的外侧关节面。外侧半月板的附加中央半脱位可使关节面几乎 100%暴露。逐步扩展入路的概念是有帮助的,应根据需要个体化进行,以实现胫骨平台骨折的解剖复位和稳定固定。