Dubner Sergio J, Teutsch Christine, Huisman Menno V, Diener Hans-Christoph, Halperin Jonathan, Rothman Kenneth J, Ma Chang-Sheng, Chuquiure-Valenzuela Eduardo, Bergler-Klein Jutta, Zint Kristina, Riou França Lionel, Lu Shihai, Paquette Miney, Lip Gregory Y H
Clínica y Maternidad Suizo Argentina, Buenos Aires, Argentina.
Boehringer Ingelheim International GmbH, Ingelheim, Germany.
ESC Heart Fail. 2020 Oct;7(5):2679-2689. doi: 10.1002/ehf2.12857. Epub 2020 Jul 2.
This study aimed to describe baseline characteristics of patients with atrial fibrillation (AF) at risk of stroke with and without history of heart failure (HF) and report 2-year outcomes in the dabigatran-treated subset of a prospective, global, observational study (GLORIA-AF).
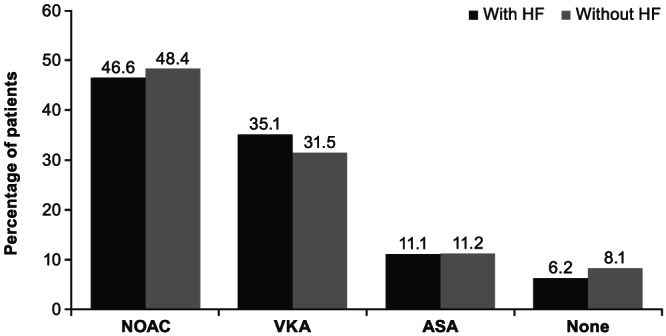
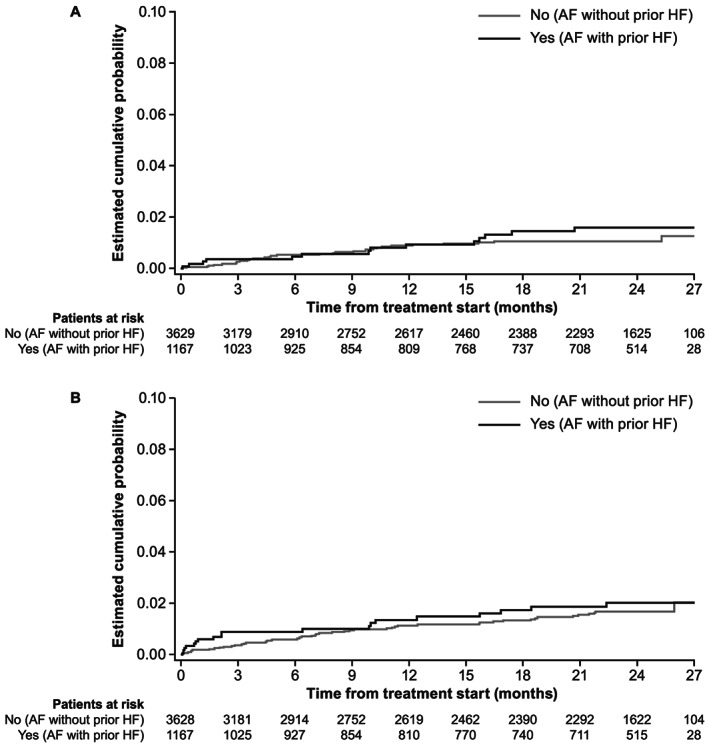
Newly diagnosed patients with AF and CHA DS -VASc score ≥ 1 were consecutively enrolled. Baseline characteristics were assessed by the presence or absence of HF diagnosis at enrolment. Incidence rates for outcomes in dabigatran-treated patients were estimated with and without standardization by stroke (excluding HF component) and bleeding risk scores. A total of 15 308 eligible patients were enrolled, including 15 154 with known HF status; of these, 3679 (24.0%) had been diagnosed with HF, 11 475 (75.0%) had not. Among 4873 dabigatran-treated patients, 1169 (24.0%) had HF, and 3658 (75.1%) did not; the risk of stroke was high (CHA DS -VASc score ≥ 2) for 94.3% of patients with HF and 85.8% without, while 6.0% and 7.0%, respectively, had a high bleeding risk (HAS-BLED ≥ 3). Incidence rates of all-cause death in dabigatran-treated patients with and without HF, standardized for CHA DS -VASc and HAS-BLED scores, were 4.76 vs. 1.80 per 100 patient years (py), with roughly comparable rates of stroke (0.82 vs. 0.60 per 100 py) and major bleeding (1.20 vs. 0.92 per 100 py).
Patients with AF and history of HF may have greater disease burden at AF diagnosis and increased mortality rates vs. patients without HF. Stroke and major bleeding rates were roughly comparable between groups confirming the long-term safety and effectiveness of dabigatran in patients with HF.
本研究旨在描述有和没有心力衰竭(HF)病史的、有卒中风险的心房颤动(AF)患者的基线特征,并报告在一项前瞻性、全球性观察性研究(GLORIA-AF)中接受达比加群治疗的亚组患者的2年结局。
连续纳入新诊断的AF患者且CHA₂DS₂-VASc评分≥1。根据入组时是否有HF诊断评估基线特征。通过卒中(不包括HF部分)和出血风险评分对接受达比加群治疗的患者的结局发生率进行标准化和未标准化估计。共纳入15308例符合条件的患者,包括15154例已知HF状态的患者;其中,3679例(24.0%)被诊断为HF,11475例(75.0%)未被诊断为HF。在4873例接受达比加群治疗的患者中,1169例(24.0%)有HF,3658例(75.1%)没有HF;94.3%有HF的患者和85.8%没有HF的患者卒中风险高(CHA₂DS₂-VASc评分≥2),而分别有6.0%和7.0%的患者出血风险高(HAS-BLED≥3)。根据CHA₂DS₂-VASc和HAS-BLED评分标准化后,接受达比加群治疗的有和没有HF的患者的全因死亡率分别为每100患者年4.76例和1.80例,卒中发生率大致相当(每100患者年0.82例和0.60例),大出血发生率也大致相当(每100患者年1.20例和0.92例)。
与没有HF病史的患者相比,有AF和HF病史的患者在AF诊断时可能有更大的疾病负担和更高的死亡率。两组之间的卒中和大出血发生率大致相当,证实了达比加群在HF患者中的长期安全性和有效性。