Department of Medicine, Memorial Sloan Kettering Cancer Center (MSKCC), 300 East 66th Street, New York, NY, 10065, USA.
Department of Medicine, Cleveland Clinic Taussig Cancer Institute, Cleveland, OH, USA.
BMC Urol. 2020 Jul 2;20(1):84. doi: 10.1186/s12894-020-00647-w.
Several phase 3 studies reported positive results for combinations of Immune-Oncology (IO) and Vascular Endothelial Growth Factor (VEGF) targeted therapies in patients with metastatic clear cell Renal Cell Carcinoma (ccRCC). However, there are limited data on outcomes to systemic therapy after IO-VEGF combinations.
A retrospective analysis was performed on patients with metastatic ccRCC treated at the Memorial Sloan Kettering Cancer Center and Cleveland Clinic who initiated systemic therapy post IO-VEGF including combinations with VEGF receptor (VEGFR) tyrosine kinase inhibitors (IO-TKI) and combinations with the anti-VEGF monoclonal antibody bevacizumab (IO-Bev). The study objectives were to evaluate the objective response rate (ORR), progression-free survival (PFS) and overall survival (OS) on systemic therapy post IO-VEGF. RECIST v1.1 criteria were used to determine radiological responses and progression. Survival estimates were evaluated with the Kaplan-Meier methods and the log-rank test from the start of systemic therapy post IO-VEGF to the event of interest.
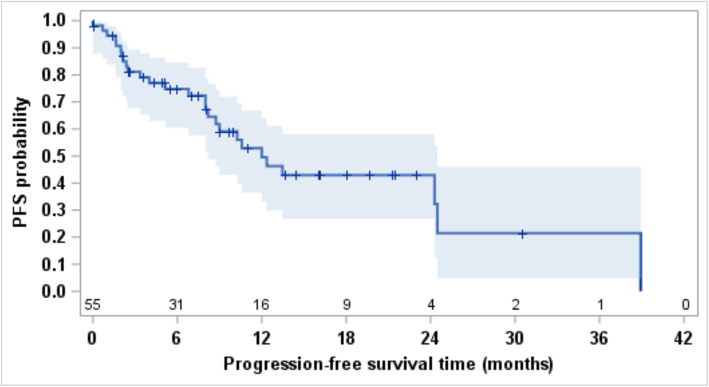
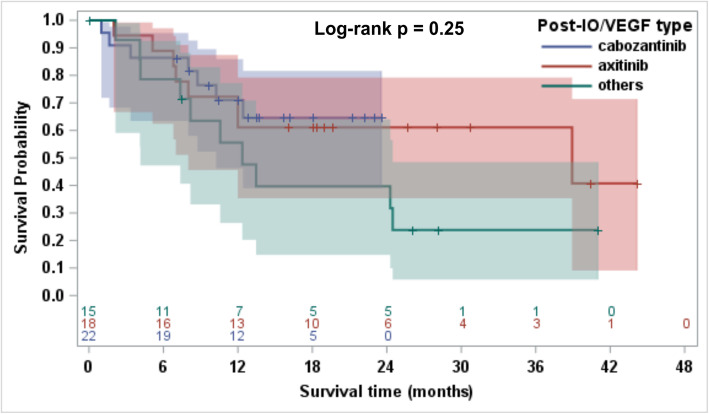
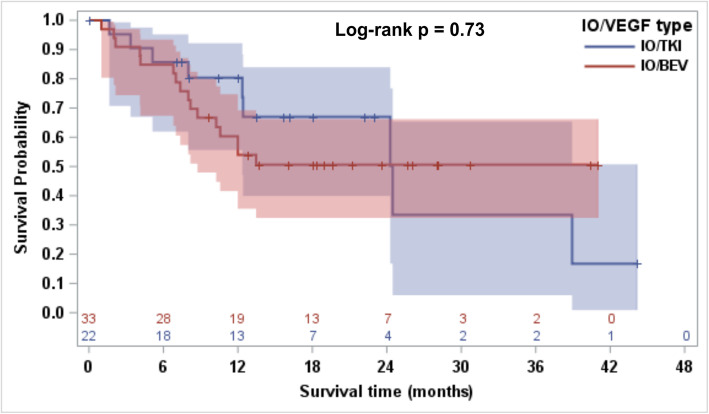
A total of fifty-nine patients were treated post discontinuation of IO-VEGF regimens which included IO-Bev (n = 35; 59%) and IO-TKI (n = 24; 41%). Fifty-eight patients (98%) received IO-VEGF regimens as part of a clinical trial. Subsequent therapies included cabozantinib (n = 22; 37%), axitinib (n = 18; 31%), pazopanib (n = 4; 7%), lenvatinib and everolimus (n = 4; 7%), mTOR inhibitor monotherapy (n = 3; 5%), axitinib and dalantercept (n = 2; 3%), sunitinib (n = 1; 2%), sorafenib (n = 1; 2%), and treatment with agents on unreported clinical trials (n = 4; 7%). Patients treated on unreported clinical trials were excluded from the efficacy analysis. Post IO-VEGF, the ORR was 25% and median PFS was 12.0 months (95% CI, 8.2-24.5). Median OS was 24.5 months (95% CI, 12-NE) and 12 months OS rate was 63.3% (95% CI, 48.6-74.9). We observed no differences post IO-VEGF OS when comparing IO- TKI vs IO-Bev (Log-rank p = 0.73).
Post IO-VEGF, most patients received VEGFR-TKIs. In this setting, VEGFR-TKIs demonstrated clinical activity and remain a viable option for salvage therapy after progression on IO-VEGF.
几项 3 期研究报告称,免疫肿瘤学(IO)和血管内皮生长因子(VEGF)靶向治疗联合治疗转移性透明细胞肾细胞癌(ccRCC)患者的结果为阳性。然而,关于 IO-VEGF 联合治疗后系统治疗的结果数据有限。
对在纪念斯隆凯特琳癌症中心和克利夫兰诊所接受治疗的转移性 ccRCC 患者进行了回顾性分析,这些患者在接受 IO-VEGF 治疗后开始接受系统治疗,包括 IO-VEGF 联合血管内皮生长因子受体(VEGFR)酪氨酸激酶抑制剂(IO-TKI)和 IO-VEGF 联合抗 VEGF 单克隆抗体贝伐珠单抗(IO-Bev)。研究目的是评估 IO-VEGF 后系统治疗的客观缓解率(ORR)、无进展生存期(PFS)和总生存期(OS)。RECIST v1.1 标准用于确定放射学反应和进展。使用 Kaplan-Meier 方法和从 IO-VEGF 后系统治疗开始到感兴趣事件的对数秩检验来评估生存估计。
共有 59 例患者在 IO-VEGF 方案停药后接受治疗,其中 IO-Bev(n=35;59%)和 IO-TKI(n=24;41%)。58 例患者(98%)接受 IO-VEGF 方案作为临床试验的一部分。随后的治疗包括卡博替尼(n=22;37%)、阿昔替尼(n=18;31%)、帕唑帕尼(n=4;7%)、仑伐替尼和依维莫司(n=4;7%)、mTOR 抑制剂单药治疗(n=3;5%)、阿昔替尼和达尔西利(n=2;3%)、舒尼替尼(n=1;2%)、索拉非尼(n=1;2%)以及接受未报告临床试验的药物治疗(n=4;7%)。接受未报告临床试验治疗的患者被排除在疗效分析之外。IO-VEGF 后,ORR 为 25%,中位 PFS 为 12.0 个月(95%CI,8.2-24.5)。中位 OS 为 24.5 个月(95%CI,12-NE),12 个月 OS 率为 63.3%(95%CI,48.6-74.9)。我们在 IO-TKI 与 IO-Bev 之间比较 IO-VEGF 后 OS 时没有观察到差异(对数秩检验 p=0.73)。
IO-VEGF 后,大多数患者接受了 VEGFR-TKI 治疗。在这种情况下,VEGFR-TKI 表现出临床活性,并且仍然是 IO-VEGF 后进展时用于挽救治疗的可行选择。