Kassab Kameel, Iskander Mina, Malhotra Saurabh, Pyslar Nataliya
Division of Cardiology, Department of Cardiology, John H. Stroger, Jr. Hospital of Cook County, 1901 W. Harrison Street, Room 3620, Chicago, IL 60612, USA.
Eur Heart J Case Rep. 2020 Apr 24;4(3):1-5. doi: 10.1093/ehjcr/ytaa089. eCollection 2020 Jun.
Giant coronary artery aneurysms (CAAs) are rare and have been reported in patients with connective tissue diseases, arteritides, and atherosclerosis. Given the rarity of the condition, multimodality imaging is essential for comprehensive evaluation of coronary aneurysms and determination of their haemodynamic significance.
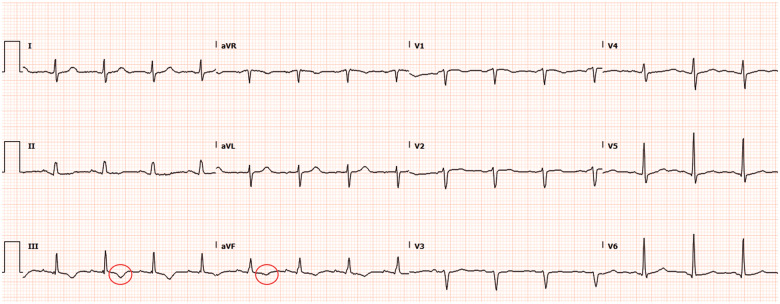
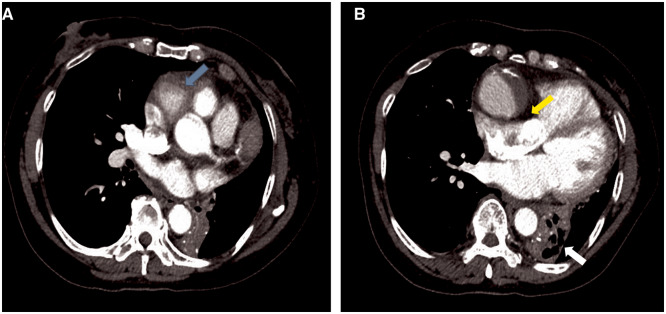
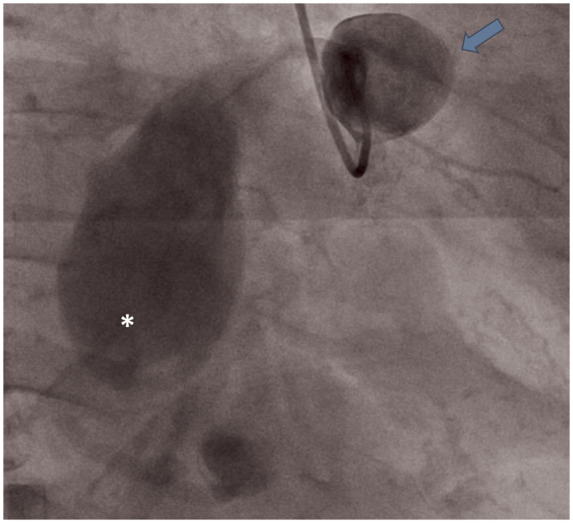
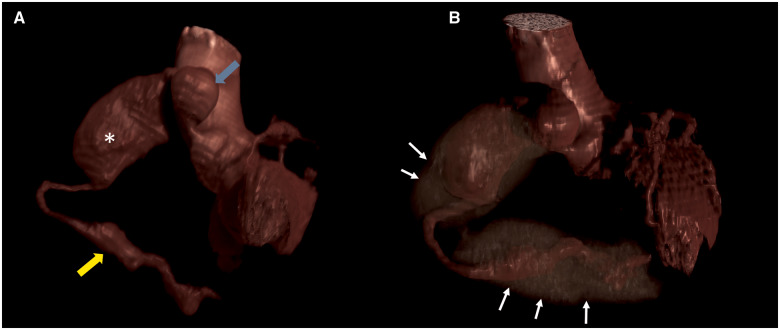
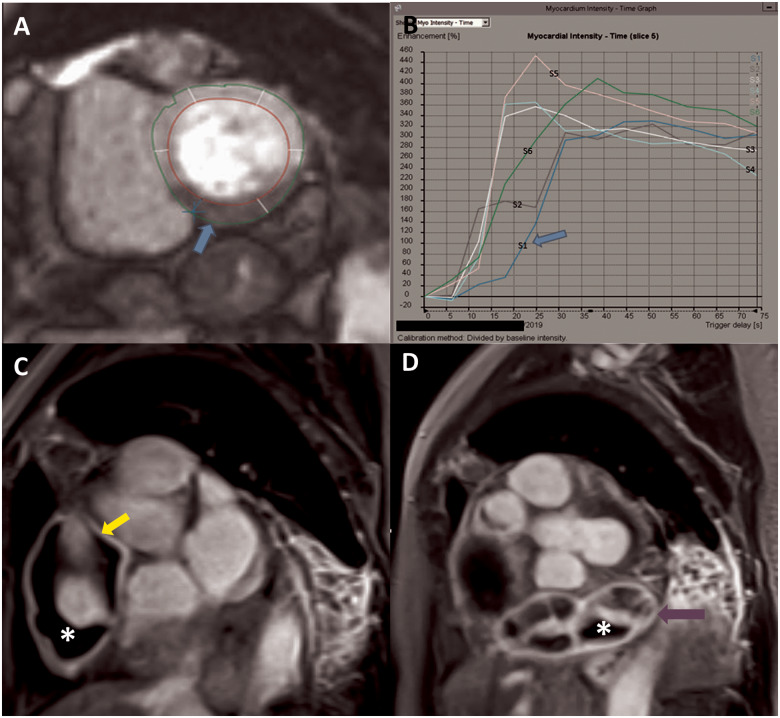
A 58-year-old Filipino female was evaluated for dyspnoea on exertion of one month. Chest computed tomography (CT) showed right coronary artery (RCA) aneurysms. Invasive coronary angiogram (ICA) confirmed two giant aneurysms of the RCA. Distal RCA could not be opacified due to contrast stagnation in the proximal aneurysms. Coronary CT angiography (CCTA) depicted an additional giant distal RCA aneurysm not visualized on ICA with intraluminal thrombosis. Contrast-enhanced cardiac magnetic resonance imaging (CMR) revealed delayed time to peak perfusion in the mid to apical inferior walls, on first-pass imaging, without myocardial scarring. Late gadolinium images revealed aneurysmal wall inflammation.
This case highlights the anatomical findings of giant CAA and the application of multimodality imaging for their accurate characterization. While ICA confirmed the presence of the aneurysms, CCTA enabled the assessment of their full extent and depict intraluminal thrombosis. Contrast-enhanced CMR delineated aneurysm wall characteristics, with first-pass images demonstrating reduced inferior wall perfusion at rest, which was likely the cause of patient's exertional symptoms. Management of giant coronary aneurysms involves surgical resection with bypass grafting.
巨大冠状动脉瘤(CAA)较为罕见,已在结缔组织病、动脉炎和动脉粥样硬化患者中报道。鉴于该病症的罕见性,多模态成像对于冠状动脉瘤的全面评估及其血流动力学意义的确定至关重要。
一名58岁的菲律宾女性因劳力性呼吸困难1个月接受评估。胸部计算机断层扫描(CT)显示右冠状动脉(RCA)瘤。有创冠状动脉造影(ICA)证实RCA有两个巨大动脉瘤。由于近端动脉瘤内造影剂滞留,RCA远端未显影。冠状动脉CT血管造影(CCTA)显示一个在ICA上未显示的额外巨大RCA远端动脉瘤,并伴有腔内血栓形成。对比增强心脏磁共振成像(CMR)显示首次通过成像时,中至心尖下壁的峰值灌注延迟,无心肌瘢痕。延迟钆增强图像显示动脉瘤壁炎症。
本病例突出了巨大CAA的解剖学发现以及多模态成像在其准确特征描述中的应用。虽然ICA证实了动脉瘤的存在,但CCTA能够评估其全貌并显示腔内血栓形成。对比增强CMR描绘了动脉瘤壁特征,首次通过图像显示静息时下壁灌注减少,这可能是患者劳力性症状的原因。巨大冠状动脉瘤的治疗包括手术切除并进行搭桥移植。