Carolina Urologic Research Center, Myrtle Beach, SC, USA.
Duke Cancer Institute, Duke University, Durham, NC, USA.
Prostate Cancer Prostatic Dis. 2024 Jun;27(2):192-201. doi: 10.1038/s41391-023-00712-z. Epub 2023 Sep 7.
Nearly one-third of patients with prostate cancer (PCa) experience biochemical recurrence (BCR) after primary definitive treatment. BCR increases the risk of distant metastasis and mortality in patients with prognostically unfavorable features. These patients are best managed with a tailored treatment strategy incorporating risk stratification using clinicopathological factors, next-generation imaging, and genomic testing.
This narrative review examines the utility of risk stratification for the management of patients with BCR in the context of clinical trial data, referencing the latest recommendations by European and US medical societies.
PubMed was searched for relevant studies published through May 21 2023 on treatment of patients with BCR after radical prostatectomy (RP) or external beam radiotherapy (EBRT).
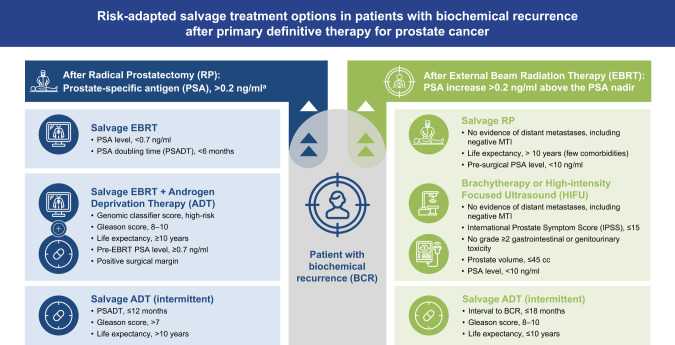
European and US guidelines support the risk-stratified management of BCR. Post-RP, salvage EBRT (with or without androgen deprivation therapy [ADT]) is an accepted treatment option for patients with BCR. Post-EBRT, local salvage therapies (RP, cryotherapy, high-intensity focused ultrasound, stereotactic body radiotherapy, and low-dose-rate and high-dose-rate brachytherapy) have demonstrated comparable relapse-free survival rates but differing adverse event profiles, short and long term. Local salvage therapies should be used for local-only relapses while ADT should be considered for regional or distant relapses. In practice, patients often receive ADT, with varying guidance for intermittent ADT vs. continuous ADT, due to consideration of quality-of-life effects.
Despite a lack of consensus for BCR treatment among guideline associations and medical societies, risk stratification of patients is essential for personalized treatment approaches, as it allows for an informed selection of therapeutic strategies and estimation of adverse events. In lower-risk disease, observation is recommended while in higher-risk disease, after failed repeat local therapy, ADT and/or clinical trial enrollment may be appropriate. Results from ongoing clinical studies of patients with BCR should provide consensus for management.
近三分之一的前列腺癌(PCa)患者在初次确定性治疗后出现生化复发(BCR)。BCR 增加了预后不良特征患者发生远处转移和死亡的风险。这些患者最好通过结合临床病理因素、下一代影像学和基因组检测进行风险分层的个体化治疗策略来进行管理。
本叙述性综述根据临床试验数据,参考欧洲和美国医学协会的最新建议,检查风险分层在管理 BCR 患者中的作用。
通过 2023 年 5 月 21 日前在 PubMed 上检索关于根治性前列腺切除术(RP)或外束放射治疗(EBRT)后 BCR 患者治疗的相关研究。
欧洲和美国的指南支持对 BCR 进行风险分层管理。RP 后,挽救性 EBRT(联合或不联合雄激素剥夺治疗 [ADT])是 BCR 患者的一种公认的治疗选择。EBRT 后,局部挽救性治疗(RP、冷冻治疗、高强度聚焦超声、立体定向体部放疗、低剂量率和高剂量率近距离放疗)已显示出可比的无复发生存率,但具有不同的不良事件特征,包括短期和长期。局部挽救性治疗应用于局部复发,而 ADT 应考虑用于区域或远处复发。在实践中,由于考虑到生活质量的影响,患者通常会接受 ADT,对间歇性 ADT 与连续性 ADT 的应用存在不同的指导意见。
尽管指南协会和医学协会之间在 BCR 治疗方面缺乏共识,但对患者进行风险分层对于个性化治疗方法至关重要,因为它可以对治疗策略进行知情选择,并估计不良事件。在低风险疾病中,建议观察;在高风险疾病中,在局部重复治疗失败后,ADT 和/或参加临床试验可能是合适的。正在进行的 BCR 患者临床研究的结果应为管理提供共识。