Department of Neurology, National Neuroscience Institute, Singapore, Singapore.
Singhealth Duke-NUS Neuroscience Academic Clinical Program, Singapore, Singapore.
BMC Neurol. 2020 Jul 7;20(1):269. doi: 10.1186/s12883-020-01846-6.
Acute ischemic stroke is a time-sensitive emergency where accurate diagnosis is required promptly. Due to time pressures, stroke mimics who present with similar signs and symptoms as acute ischemic stroke, pose a diagnostic challenge to the emergency physician. With limited access to investigative tools, clinical prediction, tools based only on clinical features, may be useful to identify stroke mimics. We aim to externally validate the performance of 4 stroke mimic prediction scales, and derive a novel decision tree, to improve identification of stroke mimics.
We performed a retrospective cross-sectional study at a primary stroke centre, served by a telestroke hub. We included consecutive patients who were administered intravenous thrombolysis for suspected acute ischemic stroke from January 2015 to October 2017. Four stroke mimic prediction tools (FABS, simplified FABS, Telestroke Mimic Score and Khan Score) were rated simultaneously, using only clinical information prior to administration of thrombolysis. The final diagnosis was ascertained by an independent stroke neurologist. Area under receiver operating curve (AUROC) analysis was performed. A classification tree analysis was also conducted using variables which were found to be significant in the univariate analysis.
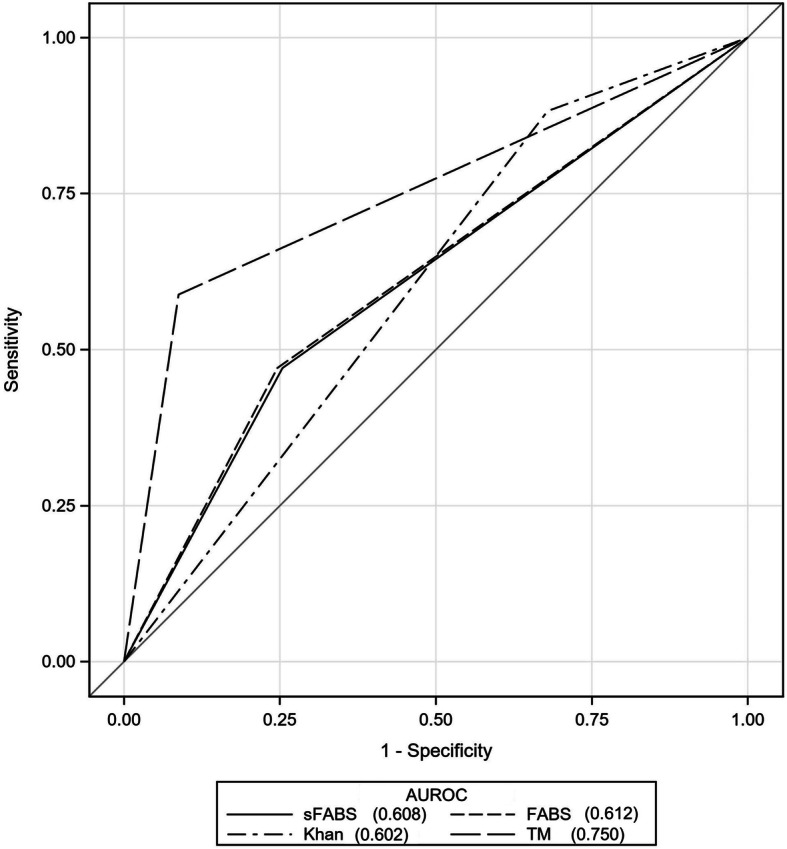
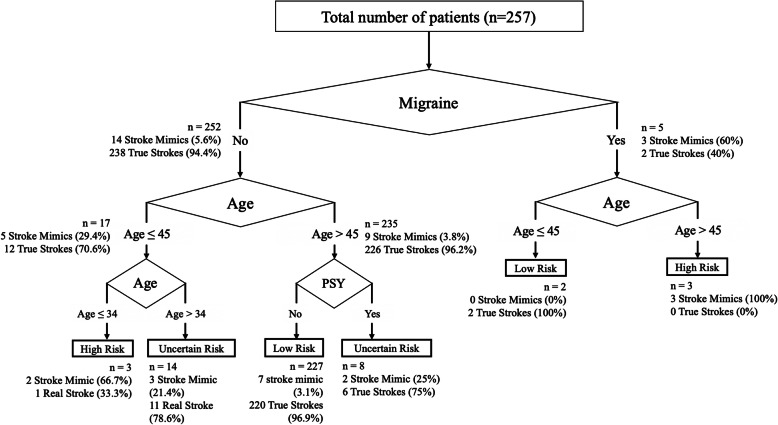
Telestroke Mimic Score had the highest discrimination for stroke mimics among the 4 scores tested (AUROC = 0.75, 95% CI = 0.63-0.87). However, all 4 scores performed similarly (DeLong p > 0.05). Telestroke Mimic Score had the highest sensitivity (91.3%), while Khan score had the highest specificity (88.2%). All 4 scores had high positive predictive value (88.1 to 97.5%) and low negative predictive values (4.7 to 32.3%). A novel decision tree, using only age, presence of migraine and psychiatric history, had a higher prediction performance (AUROC = 0.80).
Four tested stroke mimic prediction scales performed similarly to identify stroke mimics in the emergency setting. A novel decision tree may improve the identification of stroke mimics.
急性缺血性脑卒中是一种时间敏感的紧急情况,需要迅速准确地诊断。由于时间紧迫,表现出与急性缺血性脑卒中相似的体征和症状的脑卒中模拟患者对急诊医生构成了诊断挑战。由于获得的检查工具有限,仅基于临床特征的临床预测工具可能有助于识别脑卒中模拟患者。我们旨在对 4 种脑卒中模拟预测量表进行外部验证,并得出一种新的决策树,以提高脑卒中模拟患者的识别能力。
我们在一家初级卒中中心进行了一项回顾性横断面研究,该中心由远程卒中中心提供服务。我们纳入了 2015 年 1 月至 2017 年 10 月间因疑似急性缺血性脑卒中而接受静脉溶栓治疗的连续患者。在给予溶栓治疗之前,仅使用临床信息,同时对 4 种脑卒中模拟预测工具(FABS、简化 FABS、远程卒中模拟评分和 Khan 评分)进行评分。最终诊断由独立的卒中神经病学家确定。采用受试者工作特征曲线(AUROC)分析进行分析。还使用单变量分析中发现的有意义的变量进行分类树分析。
在测试的 4 种评分中,远程卒中模拟评分对脑卒中模拟患者的鉴别能力最高(AUROC=0.75,95%CI=0.63-0.87)。然而,这 4 种评分的表现均相似(DeLong p>0.05)。远程卒中模拟评分的敏感性最高(91.3%),而 Khan 评分的特异性最高(88.2%)。所有 4 种评分的阳性预测值均较高(88.1%至 97.5%),阴性预测值均较低(4.7%至 32.3%)。仅使用年龄、偏头痛存在和精神病史的新决策树具有更高的预测性能(AUROC=0.80)。
在急诊环境中,4 种测试的脑卒中模拟预测量表在识别脑卒中模拟患者方面表现相似。新的决策树可能会提高脑卒中模拟患者的识别能力。