Patsatsi Aikaterini, Uy Cybill Dianne C, Murrell Dedee F
2nd Dermatology Department, Aristotle University School of Medicine, Thessaloniki, Greece.
Department of Dermatology, University of New South Wales, Sydney, Australia.
Int J Womens Dermatol. 2020 Apr 1;6(3):199-202. doi: 10.1016/j.ijwd.2020.03.045. eCollection 2020 Jun.
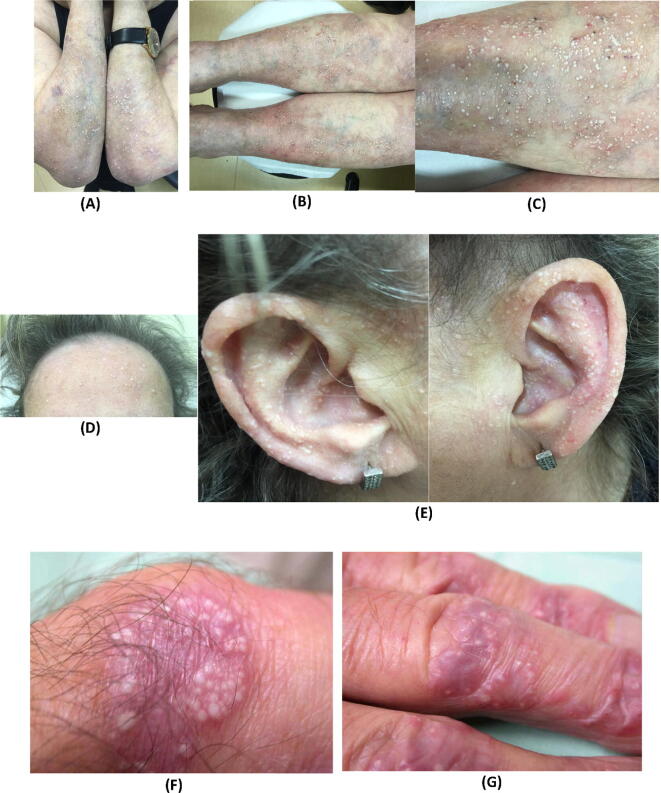
Milia are superficial keratinous cysts seen as pearly white, dome-shaped lesions 1-2 mm in diameter. Milia are associated with diseases that cause subepidermal blistering, such as hereditary forms of epidermolysis bullosa, epidermolysis bullosa acquisita, bullous pemphigoid, bullous lichen planus, and porphyria cutanea tarda. Multiple eruptive milia are rare and more extensive in number than primary milia.
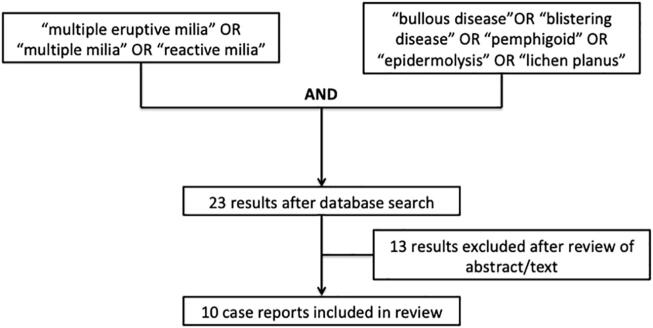
The aim of this study was to search the literature for cases of blistering diseases with multiple milia formation, especially in areas of the skin where there was no evidence of blistering or trauma, and review the interpretations of their pathogenesis.
We performed a literature search with the terms multiple milia and bullous diseases, pemphigoid, and pemphigus.
Very few studies have investigated the origin of milia. Primary milia are thought to originate from the sebaceous collar of vellus hairs, and secondary milia are believed to derive from eccrine ducts more commonly than from overlying epidermis, hair follicles, or sebaceous ducts. Milia secondary to blisters or trauma are speculated to be produced through the regeneration process of disrupted sweat glands or hair follicles. Immunological predisposition, aberrant interaction between the hemidesmosomes, and the extracellular matrix components beneath the hemidesmosomes have been described with regard to the formation of numerous milia during recovery. Multiple milia could be a primary manifestation of dystrophic epidermolysis bullosa in skin areas without evidence of blistering.
The exact etiology of multiple milia remains unknown. Immunological predisposition and improper interaction between hemidesmosomes and extracellular matrix components are speculated to play a role in the formation of milia during recovery of bullous lesions in blistering diseases. Still, further studies on the triggering mechanisms of keratinocyte dysfunction in cases of multiple milia formation without evidence of prior blistering are needed.
粟丘疹是一种浅表性角质囊肿,表现为直径1 - 2毫米的珍珠白色圆顶状损害。粟丘疹与导致表皮下水疱形成的疾病相关,如遗传性大疱性表皮松解症、获得性大疱性表皮松解症、大疱性类天疱疮、大疱性扁平苔藓和迟发性皮肤卟啉病。多发性发疹性粟丘疹较为罕见,数量比原发性粟丘疹更多且分布更广泛。
本研究旨在检索文献中关于形成多发性粟丘疹的水疱性疾病病例,尤其是在无水疱或创伤证据的皮肤区域,并综述其发病机制的相关解释。
我们使用“多发性粟丘疹”和“水疱性疾病”“类天疱疮”及“天疱疮”等术语进行文献检索。
极少有研究探讨粟丘疹的起源。原发性粟丘疹被认为起源于毳毛的皮脂腺鞘,继发性粟丘疹据信更常见于源自外分泌汗腺导管,而非上方的表皮、毛囊或皮脂腺导管。水疱或创伤继发的粟丘疹推测是通过受损汗腺或毛囊的再生过程产生的。关于恢复过程中众多粟丘疹的形成,已描述了免疫易感性、半桥粒之间以及半桥粒下方细胞外基质成分之间的异常相互作用。多发性粟丘疹可能是营养不良性大疱性表皮松解症在无水疱证据的皮肤区域的主要表现。
多发性粟丘疹的确切病因尚不清楚。推测免疫易感性以及半桥粒与细胞外基质成分之间的不当相互作用在水疱性疾病水疱性损害恢复过程中粟丘疹的形成中起作用。然而,对于无先前水疱证据的多发性粟丘疹形成病例中角质形成细胞功能障碍的触发机制仍需进一步研究。