Medical school, University of Western Australia, Perth, Australia.
School of Medicine and Pharmacology, Western Australian Centre for Health and Ageing, University of Western Australia , Perth, Australia.
BMC Geriatr. 2020 Jul 8;20(1):236. doi: 10.1186/s12877-020-01634-4.
Frail older adults living in residential aged care facilities (RACFs) usually experience comorbidities and are frequently prescribed multiple medications. This increases the potential risk of inappropriate prescribing and its negative consequences. Thus, optimising prescribed medications in RACFs is a challenge for healthcare providers.
Our aim was to systematically review interventions that increase the appropriateness of medications used in RACFs and the outcomes of these interventions.
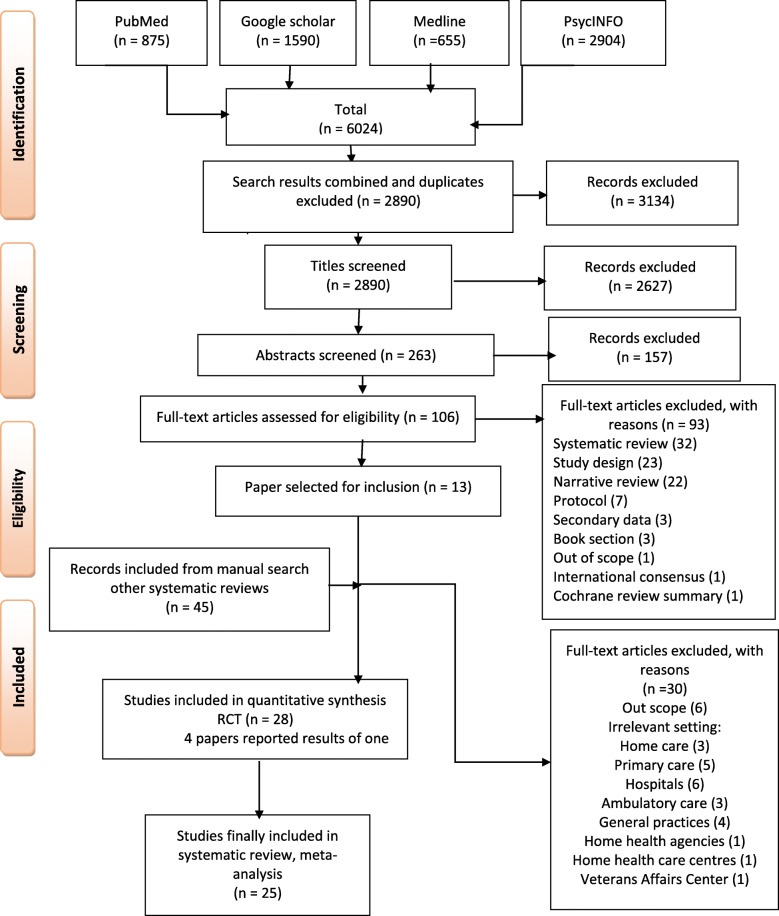
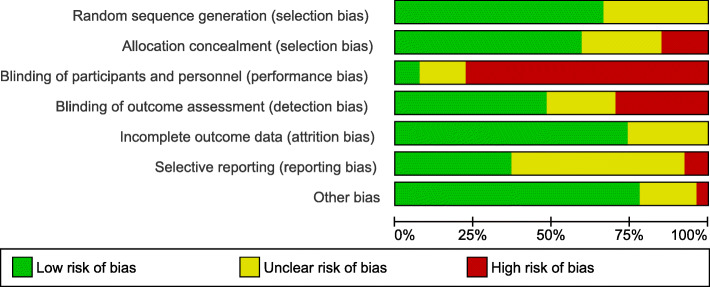
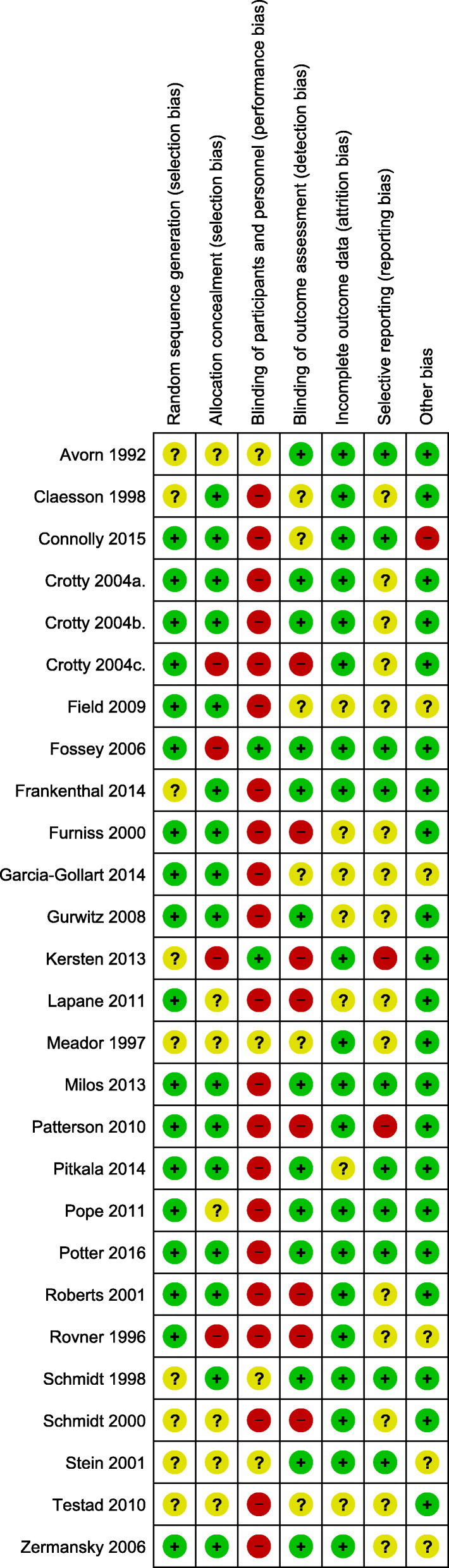
Systematic review and meta-analysis of randomised control trials (RCTs) and cluster randomised control trials (cRCTs) were performed by searching specified databases (MEDLINE, PubMed, Google scholar, PsycINFO) for publications from inception to May 2019 based on defined inclusion criteria. Data were extracted, study quality was assessed and statistically analysed using RevMan v5.3. Medication appropriateness, hospital admissions, mortality, falls, quality of life (QoL), Behavioural and Psychological Symptoms of Dementia (BPSD), adverse drug events (ADEs) and cognitive function could be meta-analysed.
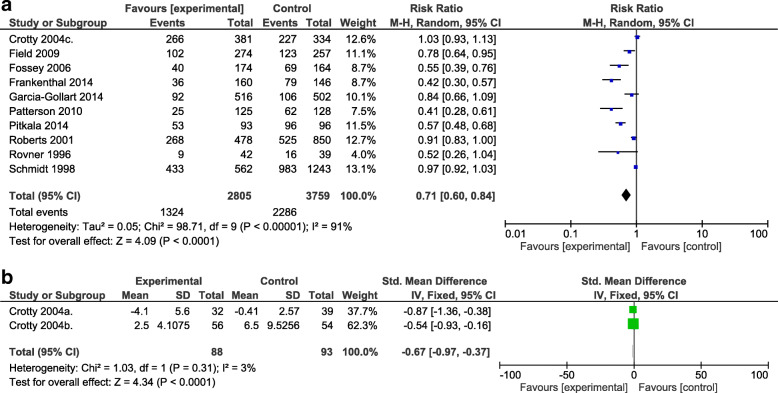
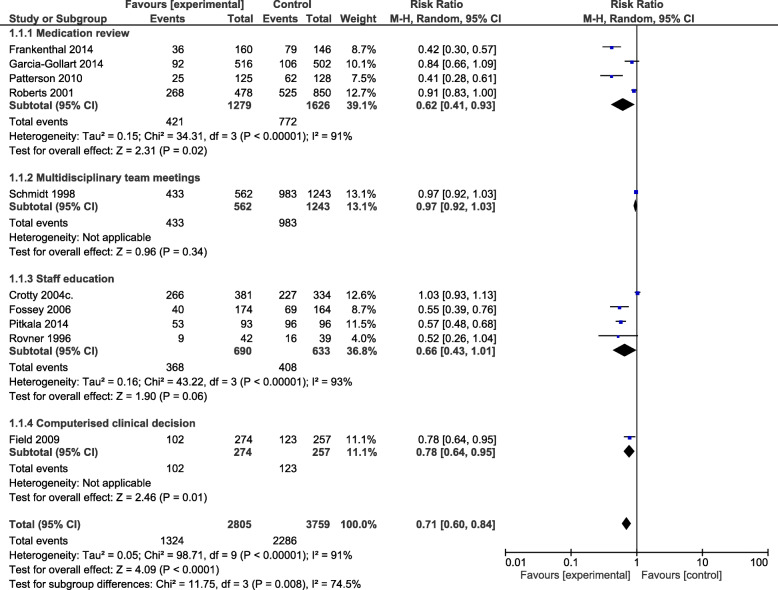
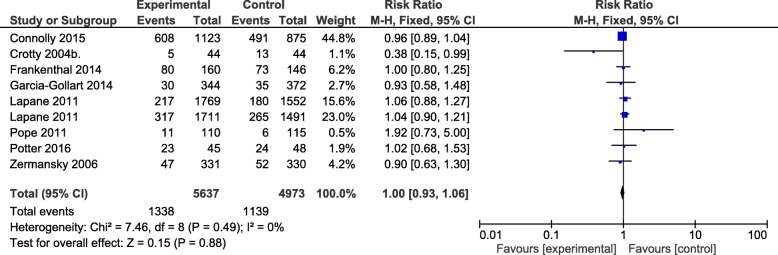
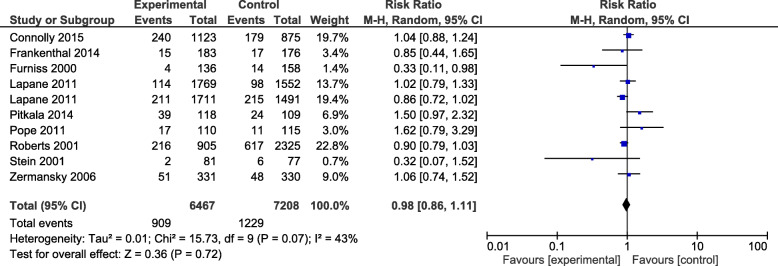
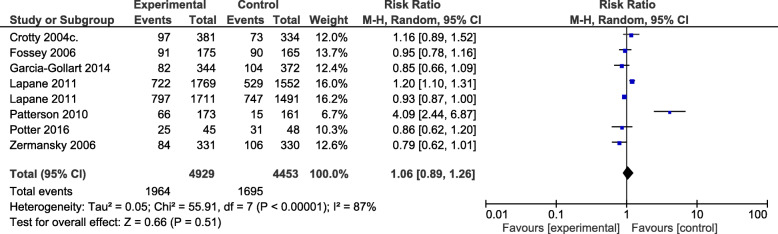
A total of 25 RCTs and cRCTs comprising 19,576 participants met the inclusion criteria. The studies tested various interventions including medication review (n = 13), staff education (n = 9), multi-disciplinary case conferencing (n = 4) and computerised clinical decision support systems (n = 2). There was an effect of interventions on medication appropriateness (RR 0.71; 95% confidence interval (CI): 0.60,0.84) (10 studies), and on medication appropriateness scales (standardised mean difference = - 0.67; 95% CI: - 0.97, - 0.36) (2 studies). There were no apparent effects on hospital admission (RR 1.00; 95% CI: 0.93, 1.06), mortality (RR 0.98; 95% CI: 0.86, 1.11), falls (RR 1.06; 95% CI: 0.89,1.26), ADEs (RR 1.04; 95% CI: 0.96,1.13), QoL (standardised mean difference = 0.16; 95% CI:-0.13, 0.45), cognitive function (weighted mean difference = 0.69; 95% CI: - 1.25, 2.64) and BPSD (RR 0.68; 95% CI: 0.44,1.06) (2 studies).
Modest improvements in medication appropriateness were observed in the studies included in this systematic review. However, the effect on clinical measures was limited to drive strong conclusions.
居住在养老院的体弱老年人通常患有合并症,并经常开多种药物。这增加了不适当处方的潜在风险及其不良后果。因此,优化养老院的处方药物对医疗保健提供者来说是一项挑战。
我们旨在系统地回顾增加养老院使用药物的适当性的干预措施及其干预措施的结果。
根据既定的纳入标准,通过在特定数据库(MEDLINE、PubMed、Google Scholar、PsycINFO)中搜索出版物,从开始到 2019 年 5 月进行了随机对照试验(RCT)和聚类随机对照试验(cRCT)的系统评价和荟萃分析。提取数据,评估研究质量,并使用 RevMan v5.3 进行统计学分析。可以对药物适当性、住院、死亡率、跌倒、生活质量(QoL)、痴呆的行为和心理症状(BPSD)、药物不良事件(ADE)和认知功能进行荟萃分析。
共有 25 项 RCT 和 cRCT 纳入了 19576 名参与者,符合纳入标准。这些研究测试了各种干预措施,包括药物审查(n=13)、员工教育(n=9)、多学科病例会议(n=4)和计算机临床决策支持系统(n=2)。干预措施对药物适当性(RR 0.71;95%置信区间(CI):0.60,0.84)(10 项研究)和药物适当性量表(标准化均数差=-0.67;95%CI:-0.97,-0.36)(2 项研究)有影响。住院(RR 1.00;95%CI:0.93,1.06)、死亡率(RR 0.98;95%CI:0.86,1.11)、跌倒(RR 1.06;95%CI:0.89,1.26)、ADE(RR 1.04;95%CI:0.96,1.13)、QoL(标准化均数差=0.16;95%CI:-0.13,0.45)、认知功能(加权均数差=0.69;95%CI:-1.25,2.64)和 BPSD(RR 0.68;95%CI:0.44,1.06)(2 项研究)没有明显的影响。
在本系统评价纳入的研究中观察到药物适当性的适度改善。然而,对临床指标的影响仅限于得出有力的结论。