Zheng Yu-Zhen, Zhai Wen-Yu, Zhao Jian, Luo Rui-Xing, Gu Wan-Jie, Fu Shen-Shen, Wu Da, Yuan Lian-Xiong, Jiang Wei, Tsutani Yasuhiro, Liao Hong-Ying, Li Xiao-Qiang
Department of Thoracic Surgery, The Sixth Affiliated Hospital, Sun Yat-sen University, Guangzhou 510655, China.
Department of Thoracic Oncology, Sun Yat-sen University Cancer Center, State Key Laboratory of Oncology in South China, Collaborative Innovation, Guangzhou 510060, China.
J Thorac Dis. 2020 Jun;12(6):3178-3187. doi: 10.21037/jtd-19-3802.
Lobectomy has long been regarded as the standard treatment for operable non-small cell lung cancer (NSCLC). Recent studies suggested that segmentectomy could achieve a good prognosis for early-stage NSCLC and might be an alternative to lobectomy in this cohort. Until now, on the issue of comparison between lobectomy and segmentectomy, there remains no published randomized controlled trial (RCT), and all existing evidence is low. Recently, a categorization of lower-level evidence has been proposed, namely, the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) system. The aim of this meta-analysis is to compare the oncologic outcome between lobectomy and segmentectomy in NSCLC with the clinical T1N0M0 stage according to the GRADE system.
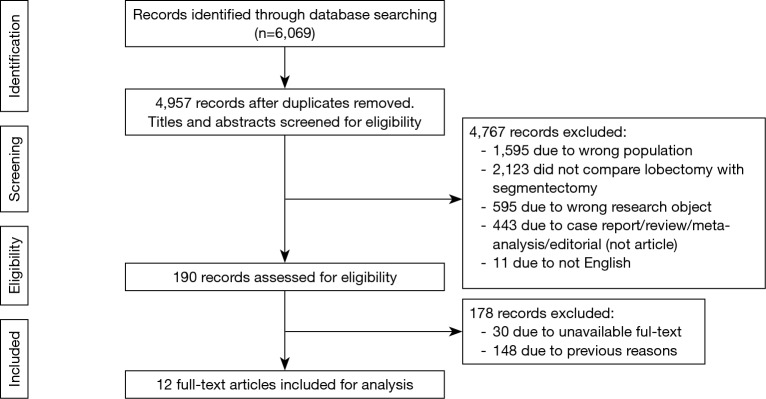
PubMed, the PMC database, EMBASE, Web of Science, and the Cochrane library were searched prior to May 2019 to identify studies that compared the prognosis between lobectomy and segmentectomy for clinical T1N0M0 NSCLC. The evidence level of the included studies was assessed according to the GRADE system, including level IIA, probably not confounded nonrandomized comparison; level IIB, possibly confounded nonrandomized comparison; and level IIC, probably confounded nonrandomized comparison. The predefined outcomes included overall survival (OS) and disease-free survival (DFS). Univariable and multivariable hazard ratios (HRs) with 95% confidence intervals (95% CI) were pooled using a random-effects model.
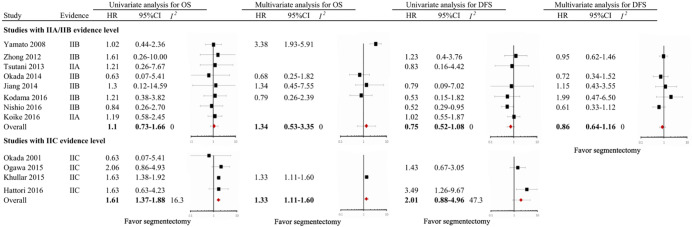
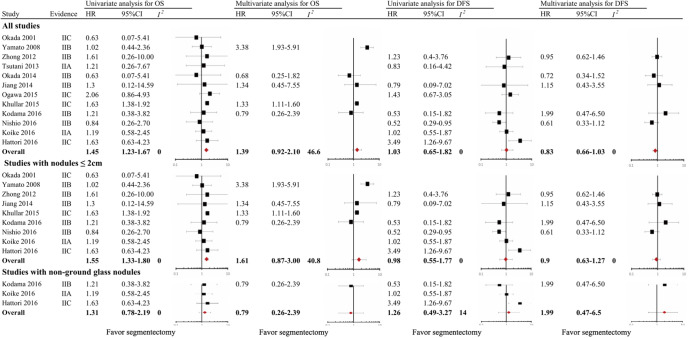
Twelve nonrandomized studies involving 8,072 participants were included. Of these studies, two were classified as IIA level (16.7%), six as IIB level (50.0%), and four as IIC level (33.3%). When crude HRs were included, compared with lobectomy, segmentectomy was associated with shorter OS but comparable DFS in the entire cohort (OS, pooled HR =1.45, 95% CI, 1.23 to 1.67; DFS, pooled HR =1.03, 95% CI, 0.65 to 1.82) and in patients with nodules ≤2 cm (OS, pooled HR =1.55, 95% CI, 1.33 to 1.80; DFS, pooled HR =0.98, 95% CI, 0.55 to 1.77). When adjusted HRs were included, the impact of segmentectomy on OS and DFS was comparable to that of lobectomy in the entire cohort (OS, pooled HR =1.39, 95% CI, 0.92 to 2.10; DFS, pooled HR =0.83, 95% CI, 0.66 to 1.03) and in patients with nodules ≤2 cm (OS, pooled HR =1.61, 95% CI, 0.87 to 3.00; DFS, pooled HR =0.90, 95% CI, 0.63 to 1.27).
Based on our results, although shorter OS is observed in patients received segmentectomy, it is necessary to wait for more results from RCT to draw a valid conclusion.
肺叶切除术长期以来一直被视为可切除非小细胞肺癌(NSCLC)的标准治疗方法。最近的研究表明,肺段切除术对于早期NSCLC可取得良好预后,在这一人群中可能是肺叶切除术的替代方案。到目前为止,在肺叶切除术和肺段切除术的比较问题上,尚无已发表的随机对照试验(RCT),所有现有证据的质量都很低。最近,有人提出了一种低级别证据的分类方法,即推荐分级、评估、制定与评价(GRADE)系统。本荟萃分析的目的是根据GRADE系统比较临床T1N0M0期NSCLC患者肺叶切除术和肺段切除术的肿瘤学结局。
在2019年5月之前检索了PubMed、PMC数据库、EMBASE、科学网和Cochrane图书馆,以确定比较临床T1N0M0期NSCLC患者肺叶切除术和肺段切除术预后的研究。根据GRADE系统评估纳入研究的证据级别,包括IIA级,可能无混杂因素的非随机对照;IIB级,可能有混杂因素的非随机对照;以及IIC级,很可能有混杂因素的非随机对照。预定义的结局包括总生存期(OS)和无病生存期(DFS)。使用随机效应模型汇总单变量和多变量风险比(HR)及95%置信区间(95%CI)。
纳入了12项涉及8072名参与者的非随机研究。在这些研究中,两项被归类为IIA级(16.7%),六项为IIB级(占50.0%),四项为IIC级(占33.3%)。纳入粗HR时,与肺叶切除术相比,在整个队列中(OS,汇总HR =1.45,95%CI为1.23至1.67;DFS,汇总HR =1.03,95%CI为0.65至1.82)以及结节≤2 cm的患者中(OS,汇总HR =1.55,95%CI为1.33至1.80;DFS,汇总HR =0.98,95%CI为0.55至1.77),肺段切除术与较短的OS相关,但DFS相当。纳入调整后的HR时,在整个队列中(OS,汇总HR =1.39,95%CI为0.92至2.10;DFS,汇总HR =0.83,95%CI为0.66至1.03)以及结节≤2 cm的患者中(OS,汇总HR =1.61,95%CI为0.87至3.00;DFS,汇总HR =0.90,95%CI为0.63至1.27),肺段切除术对OS和DFS的影响与肺叶切除术相当。
根据我们的研究结果,虽然接受肺段切除术的患者观察到较短的OS,但有必要等待更多RCT的结果才能得出有效的结论。