Kamo Yuki, Fujimoto Shinichiro, Aoshima Chihiro, Kawaguchi Yuko O, Nozaki Yui, Kudo Ayako, Takahashi Daigo, Takamura Kazuhisa, Hiki Makoto, Tomizawa Nobuo, Kumamaru Kanako K, Aoki Shigeki, Daida Hiroyuki
Department of Cardiovascular Medicine, Juntendo University Graduate School of Medicine, Tokyo, Japan.
Department of Radiology, Juntendo University Graduate School of Medicine, Tokyo, Japan.
Int J Cardiol Heart Vasc. 2020 Jul 1;29:100571. doi: 10.1016/j.ijcha.2020.100571. eCollection 2020 Aug.
The concept of active atherosclerotic disease has been accepted for heart valve calcification (HVC). We investigated prevalence, distribution and related factors of HVC in patients who had undergone coronary CT angiography (CCTA).
Subjects were consecutive 200 patients who underwent CCTA. The prevalence and the distribution of HVC using ECG gated non-contrast CT were investigated. Logistic regression analysis and simple regression analysis for factors associated with presence of the calcification and quantitative calcification in the aortic and mitral valve were conducted.
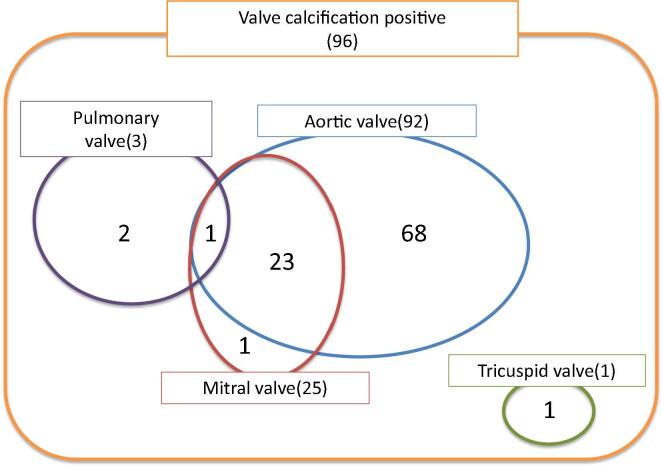
HVC was detected in 48.0%. Aortic valve calcification (AVC) was found in 92 cases, the most, followed by mitral valve calcification (MVC) in 25 cases, pulmonary valve in 3 cases, and tricuspid valve in 1 case. Although the left coronary cusp showed the most in 65.2%, no statistic significant difference for Agatston score was detected among each cusp in AVC. Multiple logistic regression analysis showed that age (OR:1.211, 95%C.I.:1.0716-1.1728, p < 0.0001) and coronary artery calcium score (CACS) grade (grade2 OR:7.3393, 95%C.I.:1.7699-30.4349, p = 0.0060, grade3 OR:7.2214, 95%C.I.:1.4376-36.2762, p = 0.0164) were significant factors associated with presence of AVC. The significant factors associated with quantitative AVC were age (p = 0.0043), dyslipidemia (p = 0.0117), and statin use (p = 0.0221). Only age (OR:1.1589, 95%C.I.:1.0726-1.2520, p = 0.0002) was significant factor related to presence of MVC. No significant related factor was found in quantitative MVC.
There was an association between presence of AVC and CACS, but not a significant association with presence of MVC. Neither quantitative AVC nor MVC had a significant association with CACS or coronary artery disease.
心脏瓣膜钙化(HVC)已被纳入动脉粥样硬化性疾病的范畴。我们调查了接受冠状动脉CT血管造影(CCTA)的患者中HVC的患病率、分布情况及相关因素。
研究对象为连续200例接受CCTA的患者。采用心电图门控非增强CT对HVC的患病率及分布情况进行调查。对主动脉瓣和二尖瓣钙化的存在及定量钙化的相关因素进行逻辑回归分析和简单回归分析。
HVC的检出率为48.0%。发现主动脉瓣钙化(AVC)92例,最为常见,其次是二尖瓣钙化(MVC)25例,肺动脉瓣钙化3例,三尖瓣钙化1例。虽然左冠状动脉瓣叶钙化最为多见,占65.2%,但AVC各瓣叶间的阿加西积分无统计学显著差异。多因素逻辑回归分析显示,年龄(OR:1.211,95%置信区间:1.0716 - 1.1728,p < 0.0001)和冠状动脉钙化积分(CACS)分级(2级OR:7.3393,95%置信区间:1.7699 - 30.4349,p = 0.0060;3级OR:7.2214,95%置信区间:1.4376 - 36.2762,p = 0.0164)是与AVC存在相关的显著因素。与定量AVC相关的显著因素为年龄(p = 0.0043)、血脂异常(p = 0.0117)和他汀类药物使用(p = 0.0221)。仅年龄(OR:1.1589,95%置信区间:1.0726 - 1.2520,p = 0.0002)是与MVC存在相关的显著因素。定量MVC未发现显著相关因素。
AVC的存在与CACS之间存在关联,但与MVC的存在无显著关联。定量AVC和MVC与CACS或冠状动脉疾病均无显著关联。