Department of General, Visceral and Transplant Surgery, Surgical Technology and Training, Tuebingen University Hospital, Waldhoernlestrasse 22, 72072, Tuebingen, Germany.
Clinic for General, Visceral and Pediatric Surgery, Duesseldorf University Hospital, Moorenstr. 5, 40225, Düsseldorf, Germany.
Surg Endosc. 2021 Jul;35(7):3303-3312. doi: 10.1007/s00464-020-07768-1. Epub 2020 Jul 8.
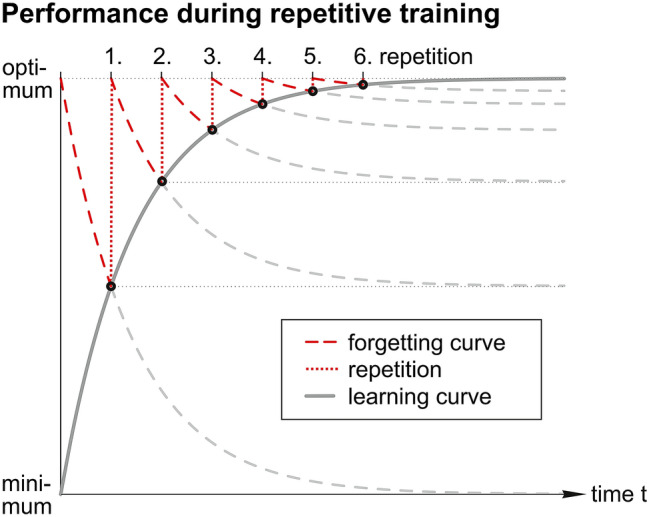
The effectiveness of practical surgical training is characterised by an inherent learning curve. Decisive are individual initial starting capabilities, learning speed, ideal learning plateaus, and resulting learning potentials. The quantification of learning curves requires reproducible tasks with varied levels of difficulty. The hypothesis of this study is that the use of three-dimensional (3D) vision is more advantageous than two-dimensional vision (2D) for the learning curve in laparoscopic training.
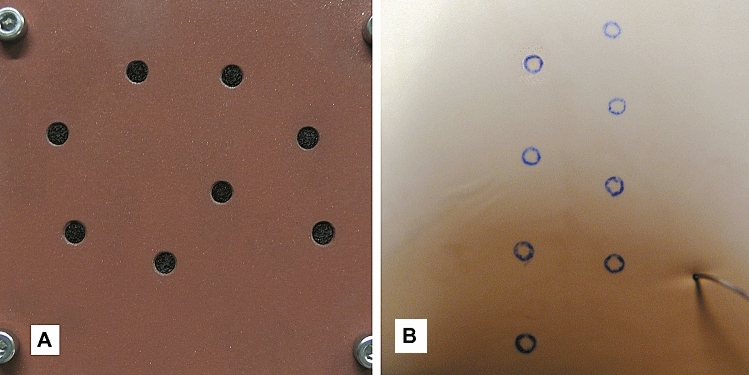
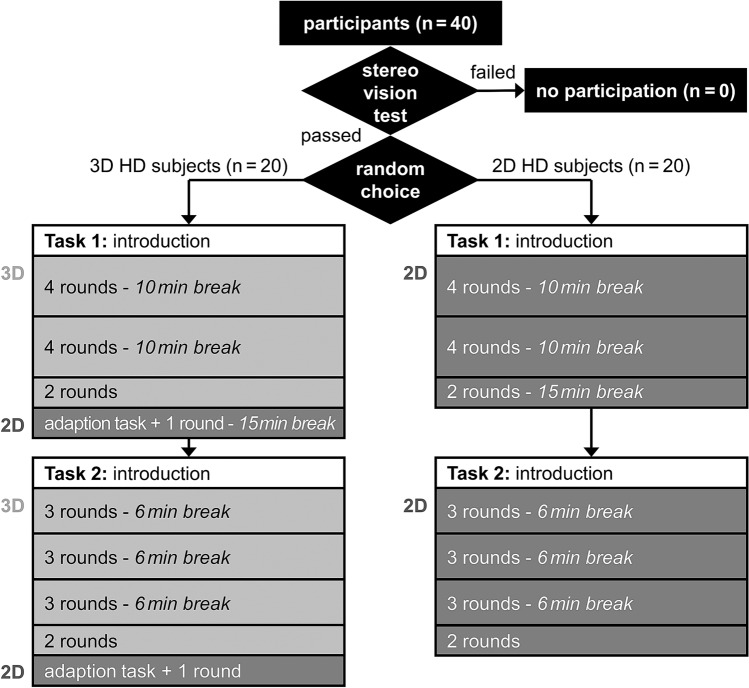
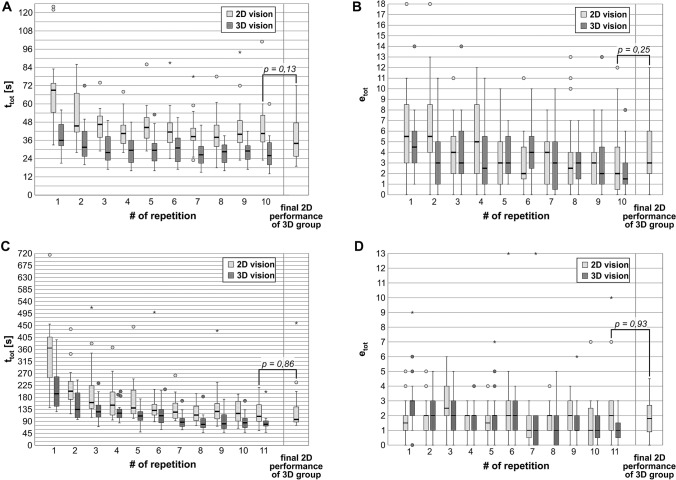
Forty laparoscopy novices were recruited and randomised to a 2D Group and a 3D Group. A laparoscopy box trainer with two standardised tasks was used for training of surgical tasks. Task 1 was a positioning task, while Task 2 called for laparoscopic knotting as a more complex process. Each task was repeated at least ten times. Performance time and the number of predefined errors were recorded. 2D performance after 3D training was assessed in an additional final 2D cycle undertaken by the 3D Group.
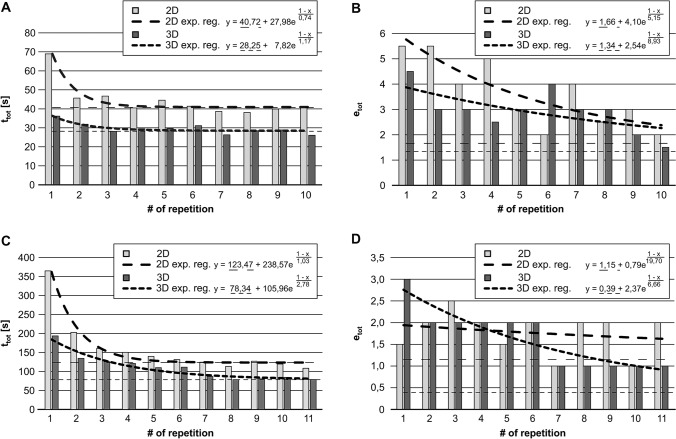
The calculated learning plateaus of both performance times and errors were lower for 3D. Independent of the vision mode the learning curves were smoother (exponential decay) and efficiency was learned faster than precision. The learning potentials varied widely depending on the corresponding initial values and learning plateaus. The final 2D performance time of the 3D-trained group was not significantly better than that of the 2D Group. The final 2D error numbers were similar for all groups.
Stereoscopic vision can speed up laparoscopic training. The 3D learning curves resulted in better precision and efficiency. The 3D-trained group did not show inferior performance in the final 2D cycle. Consequently, we encourage the training of surgical competences like suturing and knotting under 3D vision, even if it is not available in clinical routine.
实际手术培训的效果具有内在的学习曲线特征。决定性因素是个人初始起点能力、学习速度、理想学习平台以及由此产生的学习潜力。学习曲线的量化需要具有不同难度水平的可重复任务。本研究的假设是,在腹腔镜培训中,使用三维(3D)视觉比二维视觉(2D)更有利于学习曲线。
招募了 40 名腹腔镜新手,并将他们随机分为 2D 组和 3D 组。使用带有两个标准化任务的腹腔镜箱式训练器进行手术任务的培训。任务 1 是定位任务,而任务 2 需要进行腹腔镜打结,这是一个更复杂的过程。每个任务至少重复十次。记录操作时间和预定错误的数量。3D 组在额外的最后一个 2D 周期中评估 2D 训练后的 2D 性能。
3D 的两个性能时间和错误的计算学习平台较低。无论视觉模式如何,学习曲线都更加平滑(指数衰减),效率的学习速度都快于精度。学习潜力因相应的初始值和学习平台而异。3D 训练组的最终 2D 操作时间并不明显优于 2D 组。所有组的最终 2D 错误数量相似。
立体视觉可以加快腹腔镜培训。3D 学习曲线导致更好的精度和效率。在最后一个 2D 周期中,3D 训练组的表现并不差。因此,即使在临床常规中不可用,我们也鼓励在 3D 视觉下进行缝合和打结等手术技能的培训。