Division of Cardiology and Cardiac Catheterization Laboratories, Showa University Northern Yokohama Hospital, 35-1, Chigasaki-Chuo, Tsuzuki, Yokohama, 224-8503, Japan.
ESC Heart Fail. 2020 Oct;7(5):2912-2921. doi: 10.1002/ehf2.12901. Epub 2020 Jul 9.
Our purpose was to investigate the association between the B-type natriuretic peptide (BNP) level at discharge, the occurrence of worsening renal function (WRF), and long-term outcomes in patients with heart failure (HF).
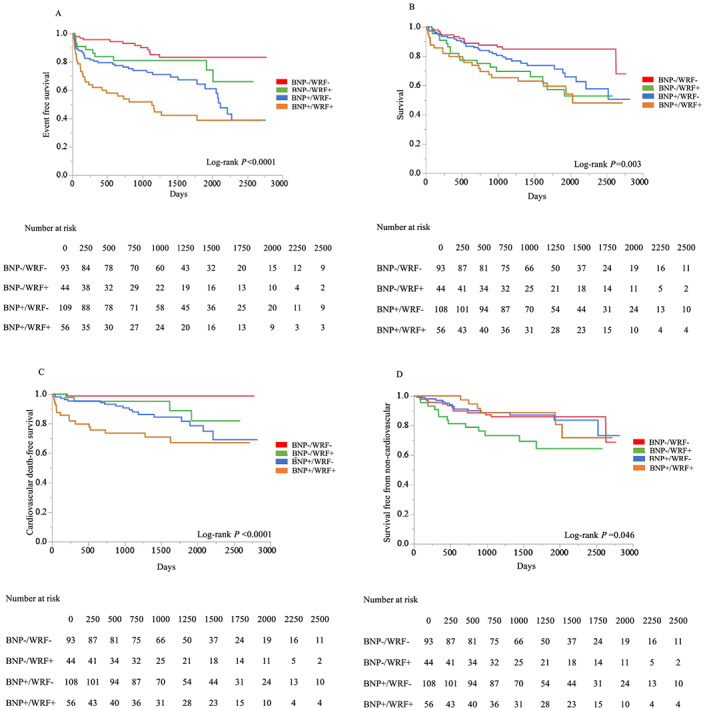
We enrolled hospitalized acute HF patients. We divided patients into four groups on the basis of BNP <250 pg/mL (BNP-) or BNP ≥250 pg/mL (BNP+) at discharge and the occurrence of WRF during admission: BNP-/WRF-, BNP-/WRF+, BNP+/WRF-, and BNP+/WRF+. We evaluated the association between BNP at discharge, WRF, and cardiovascular/all-cause mortality/hospitalization due to HF. Clinical follow-up was completed in 301 patients. At discharge, percentages of the patients with clinical signs of HF were low and similar among four groups. The median follow-up period was 1206 days (interquartile range, 733-1825 days). The composite endpoint of cardiovascular mortality and HF hospitalization was significantly different between the four groups [12.9% (BNP-/WRF-), 22.7% (BNP-/WRF+), 35.8% (BNP+/WRF-), and 55.4% (BNP+/WRF+), P < 0.0001]. All-cause mortality was also different etween the four groups (15.1%, 38.6%, 28.7%, and 39.3%, respectively, P = 0.003). In the multivariate Cox proportional hazards model, the combination of BNP ≥250 pg/mL and WRF showed the highest hazard ratio (HR) for composite endpoint (HR, 5.201; 95% confidence interval, 2.582-11.11; P < 0.0001), and BNP-/WRF+ was associated with increased all-cause mortality (HR, 2.286; 95% confidence interval, 1.089-4.875; P = 0.03). Patients in BNP+/WRF+ had a higher cardiovascular mortality (28.6%), and those in BNP-/WRF+ had a high non-cardiovascular mortality (29.5%).
Heart failure patients with BNP ≥250 pg/mL at discharge and in-hospital occurrence of WRF had the highest risk for the composite endpoint (cardiovascular mortality and HF hospitalization) among groups.
本研究旨在探讨心力衰竭(HF)患者出院时 B 型利钠肽(BNP)水平、肾功能恶化(WRF)的发生与长期预后之间的关系。
我们纳入了住院的急性 HF 患者。根据出院时 BNP<250pg/mL(BNP-)或 BNP≥250pg/mL(BNP+)以及住院期间 WRF 的发生情况,我们将患者分为四组:BNP-/WRF-、BNP-/WRF+、BNP+/WRF-和 BNP+/WRF+。我们评估了出院时 BNP、WRF 与心血管/全因死亡率/HF 再住院之间的关系。301 例患者完成了临床随访。出院时,四组患者的 HF 临床体征发生率较低且相似。中位随访时间为 1206 天(四分位距 733-1825 天)。心血管死亡率和 HF 住院的复合终点在四组之间差异有统计学意义[12.9%(BNP-/WRF-)、22.7%(BNP-/WRF+)、35.8%(BNP+/WRF-)和 55.4%(BNP+/WRF+),P<0.0001]。四组之间的全因死亡率也不同(分别为 15.1%、38.6%、28.7%和 39.3%,P=0.003)。多变量 Cox 比例风险模型显示,BNP≥250pg/mL 联合 WRF 对复合终点的风险比(HR)最高(HR,5.201;95%置信区间,2.582-11.11;P<0.0001),且 BNP-/WRF+与全因死亡率增加相关(HR,2.286;95%置信区间,1.089-4.875;P=0.03)。BNP+/WRF+组患者的心血管死亡率较高(28.6%),而 BNP-/WRF+组患者的非心血管死亡率较高(29.5%)。
出院时 BNP≥250pg/mL 且住院期间发生 WRF 的 HF 患者发生复合终点(心血管死亡率和 HF 住院)的风险最高。