Department of Mathematics and Statistics, York University, Toronto, M3J 1P3, Canada.
Laboratory for Industrial and Applied Mathematics, York University, Toronto, M3J 1P3, ON, Canada.
Theor Biol Med Model. 2020 Jul 10;17(1):11. doi: 10.1186/s12976-020-00129-4.
Seasonal influenza poses a significant public health and economic burden, associated with the outcome of infection and resulting complications. The true burden of the disease is difficult to capture due to the wide range of presentation, from asymptomatic cases to non-respiratory complications such as cardiovascular events, and its seasonal variability. An understanding of the magnitude of the true annual incidence of influenza is important to support prevention and control policy development and to evaluate the impact of preventative measures such as vaccination.
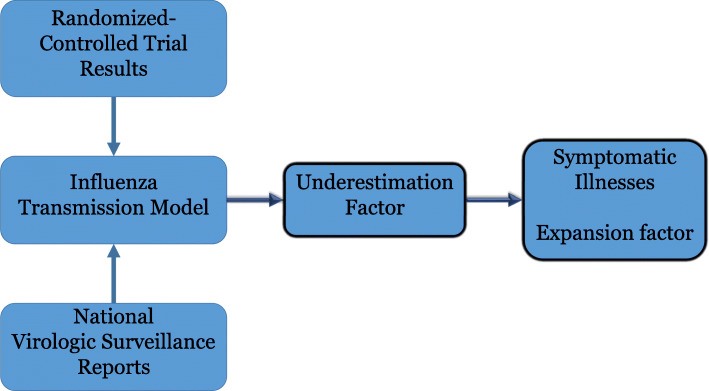
We use a dynamic disease transmission model, laboratory-confirmed influenza surveillance data, and randomized-controlled trial (RCT) data to quantify the underestimation factor, expansion factor, and symptomatic influenza illnesses in the US and Canada during the 2011-2012 and 2012-2013 influenza seasons.
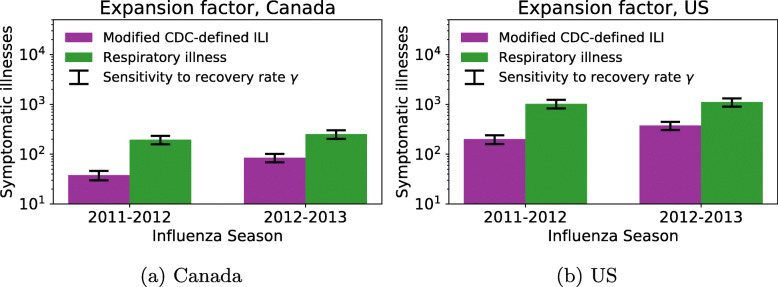
Based on 2 case definitions, we estimate between 0.42-3.2% and 0.33-1.2% of symptomatic influenza illnesses were laboratory-confirmed in Canada during the 2011-2012 and 2012-2013 seasons, respectively. In the US, we estimate between 0.08-0.61% and 0.07-0.33% of symptomatic influenza illnesses were laboratory-confirmed in the 2011-2012 and 2012-2013 seasons, respectively. We estimated the symptomatic influenza illnesses in Canada to be 0.32-2.4 million in 2011-2012 and 1.8-8.2 million in 2012-2013. In the US, we estimate the number of symptomatic influenza illnesses to be 4.4-34 million in 2011-2012 and 23-102 million in 2012-2013.
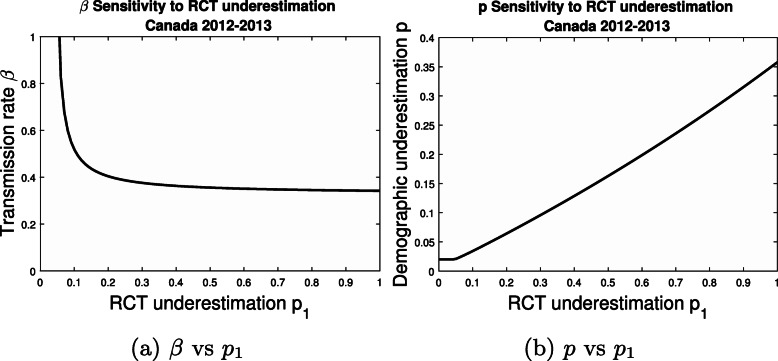
We illustrate that monitoring a representative group within a population may aid in effectively modelling the transmission of infectious diseases such as influenza. In particular, the utilization of RCTs in models may enhance the accuracy of epidemiological parameter estimation.
季节性流感对公共卫生和经济造成重大负担,与感染结果和由此产生的并发症有关。由于临床表现广泛,从无症状病例到心血管事件等非呼吸道并发症,以及其季节性变化,因此很难准确捕捉疾病的真实负担。了解流感真实年发病率的程度对于支持预防和控制政策的制定以及评估疫苗接种等预防措施的影响非常重要。
我们使用动态疾病传播模型、实验室确诊的流感监测数据和随机对照试验 (RCT) 数据来量化美国和加拿大在 2011-2012 年和 2012-2013 年流感季节的低估因素、扩展因素和有症状的流感病例。
根据两种病例定义,我们估计加拿大在 2011-2012 年和 2012-2013 年季节中,有症状流感病例中有 0.42-3.2%和 0.33-1.2%经过实验室确诊。在美国,我们估计 2011-2012 年和 2012-2013 年季节中,有症状流感病例中有 0.08-0.61%和 0.07-0.33%经过实验室确诊。我们估计加拿大在 2011-2012 年有 0.32-2.400 万例有症状流感病例,在 2012-2013 年有 1.8-8.200 万例有症状流感病例。在美国,我们估计 2011-2012 年有 4.4-3400 万例有症状流感病例,在 2012-2013 年有 23-10200 万例有症状流感病例。
我们说明,在人群中监测代表性群体可以帮助有效模拟流感等传染病的传播。特别是,在模型中利用 RCT 可以提高流行病学参数估计的准确性。