Ortiz Justin R, Neuzil Kathleen M, Shay David K, Rue Tessa C, Neradilek Moni B, Zhou Hong, Seymour Christopher W, Hooper Laura G, Cheng Po-Yung, Goss Christopher H, Cooke Colin R
1Department of Medicine, University of Washington, Seattle, WA. 2Department of Global Health, University of Washington, Seattle, WA. 3Vaccine Access and Delivery Global Program, PATH, Seattle, WA. 4Influenza Division, Centers for Disease Control and Prevention, Centers for Disease Prevention and Control, Atlanta, GA. 5Department of Biostatistics, University of Washington, Seattle, WA. 6The Mountain-Whisper-Light Statistics, Seattle, WA. 7Division of Health Informatics and Surveillance (proposed), Centers for Disease Prevention and Control, Atlanta, GA. 8Departments of Critical Care and Emergency Medicine, University of Pittsburgh, Pittsburgh, PA. 9Department of Medicine, University of Michigan, Ann Arbor, MI.
Crit Care Med. 2014 Nov;42(11):2325-32. doi: 10.1097/CCM.0000000000000545.
Influenza is the most common vaccine-preventable disease in the United States; however, little is known about the burden of critical illness due to influenza virus infection. Our primary objective was to estimate the proportion of all critical illness hospitalizations that are attributable to seasonal influenza.
Retrospective cohort study.
Arizona, California, and Washington from January 2003 to March 2009.
All adults hospitalized with critical illness, defined by International Classification of Diseases, 9th Edition, Clinical Modification diagnosis and procedure codes for acute respiratory failure, severe sepsis, or in-hospital death.
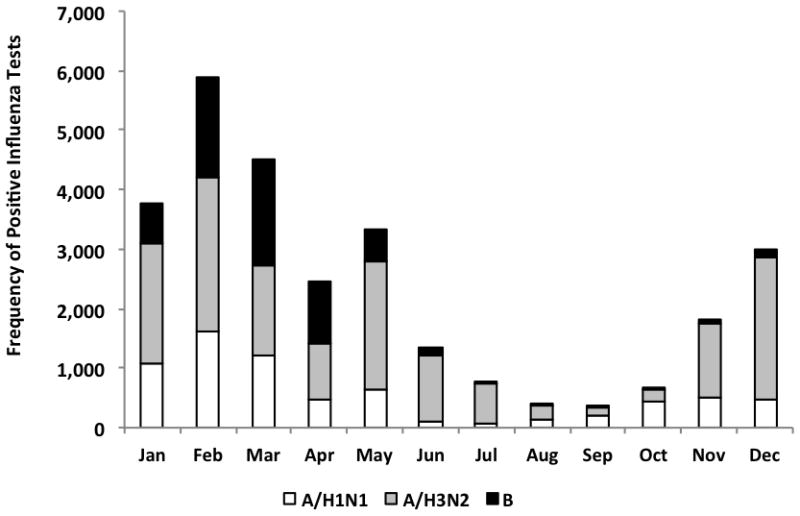
We combined the complete hospitalization discharge databases for three U.S. states, regional influenza virus surveillance, and state census data. Using negative binomial regression models, we estimated the incidence rates of adult influenza-associated critical illness hospitalizations and compared them with all-cause event rates. We also compared modeled outcomes to International Classification of Diseases, 9th Edition, Clinical Modification-coded influenza hospitalizations to assess potential underrecognition of severe influenza disease. During the study period, we estimated that 26,760 influenza-associated critical illness hospitalizations (95% CI, 14,541, 47,464) occurred. The population-based incidence estimate for influenza-associated critical illness was 12.0 per 100,000 person-years (95% CI, 6.6, 21.6) or 1.3% of all critical illness hospitalizations (95% CI, 0.7%, 2.3%). During the influenza season, 3.4% of all critical illness hospitalizations (95% CI, 1.9%, 5.8%) were attributable to influenza. There were only 2,612 critical illness hospitalizations with International Classification of Diseases, 9th Edition, Clinical Modification-coded influenza diagnoses, suggesting influenza is either undiagnosed or undercoded in a substantial proportion of critical illness.
Extrapolating our data to the 2010 U.S. population, we estimate that about 28,000 adults are hospitalized for influenza-associated critical illness annually. Influenza in many of these critically ill patients may be undiagnosed. Critical care physicians should have a high index of suspicion for influenza in the ICU, particularly when influenza is known to be circulating in their communities.
流感是美国最常见的可通过接种疫苗预防的疾病;然而,关于流感病毒感染所致危重症负担的了解却很少。我们的主要目的是估计所有因季节性流感导致的危重症住院病例的比例。
回顾性队列研究。
2003年1月至2009年3月期间的亚利桑那州、加利福尼亚州和华盛顿州。
所有因危重症住院的成年人,根据《国际疾病分类》第9版临床修订本中急性呼吸衰竭、严重脓毒症或院内死亡的诊断和操作编码确定。
我们合并了美国三个州完整的住院出院数据库、地区流感病毒监测数据和州人口普查数据。使用负二项回归模型,我们估计了成人流感相关危重症住院的发病率,并将其与全因事件发生率进行比较。我们还将模型结果与《国际疾病分类》第9版临床修订本编码的流感住院病例进行比较,以评估严重流感疾病可能存在的诊断不足情况。在研究期间,我们估计发生了26,760例流感相关危重症住院病例(95%置信区间,14,541至47,464)。基于人群的流感相关危重症发病率估计为每10万人年12.0例(95%置信区间,6.6至21.6),占所有危重症住院病例的1.3%(95%置信区间,0.7%,2.3%)。在流感季节,所有危重症住院病例中有3.4%(95%置信区间,1.9%,5.8%)可归因于流感。仅有2,612例危重症住院病例的《国际疾病分类》第9版临床修订本编码为流感诊断,这表明在相当一部分危重症病例中,流感要么未被诊断,要么编码不足。
将我们的数据外推至2010年美国人口,我们估计每年约有28,000名成年人因流感相关危重症住院。这些危重症患者中的许多人感染的流感可能未被诊断出来。重症监护医生在重症监护病房应对流感保持高度怀疑,尤其是当已知流感在其所在社区传播时。