Cai Xianlei, Zhang Miaozun, Liang Chao, Xu Yuan, Yu Weiming
Department of Gastrointestinal Surgery, Ningbo Medical Center Lihuili Hospital, 57 Xingning Road, 315000, Ningbo, PR China.
BMC Surg. 2020 Jul 9;20(1):149. doi: 10.1186/s12893-020-00809-5.
Delayed gastric emptying (DGE) is a common and frustrating complication of pancreaticoduodenectomy (PD). Studies suggest that surgical methods and other clinical characteristics may affect the occurrence of DGE. Nevertheless, the results of such studies are conflicting. The objective of this work was to perform a propensity score matching analysis to compare the differences between pylorus-preserving pancreaticoduodenectomy (PPPD) and pylorus-removing pancreaticoduodenectomy (PrPD) and to develop and validate a nomogram to predict the probability of severe DGE (SDGE).
This retrospective study enrolled patients who underwent PD at our institution from December 2009 to December 2018. Propensity score matching was applied at a ratio of 1:1 to compare PPPD and PrPD groups. We compared incidence of complications, DGE, lengths of hospital stay, hospitalization costs, and mortality. Univariate and multivariate logistic regression analysis were performed to identify potential risk factors of severe DGE. Finally, a nomogram was developed and validated to predict severe DGE.
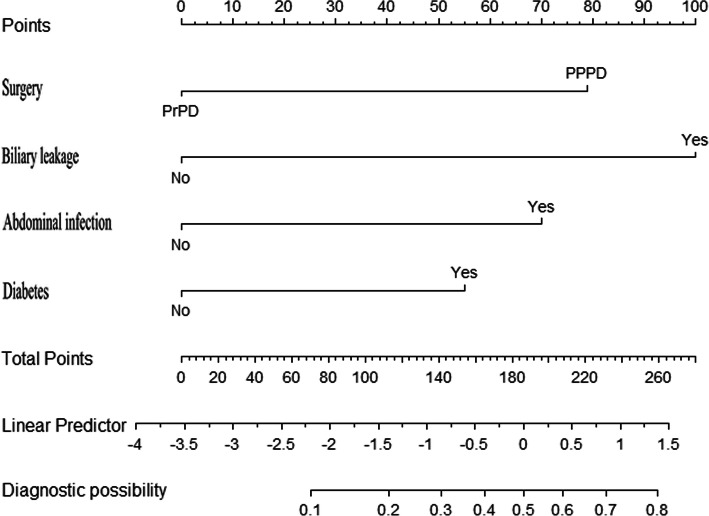
The PPPD group had a significantly higher rate of postoperative pancreatic fistula (29.9% versus 17.4%, P < 0.05) and less blood loss (463.7 ml versus 694.9 ml, P < 0.05). After propensity score matching, the PPPD group had a significantly higher rate of postoperative DGE (19.2% versus 3.8%, P < 0.05), especially severe DGE (17.3% versus 0%) than the PrPD group. There were no significant differences in terms of lengths of hospital stay, hospitalization costs or mortality between the groups. Surgical method, biliary leakage, abdominal infection, and diabetes were independent risk factors for SDGE. The nomogram predicted SDGE with a training C - index of 0.798 and a validation C - index of 0.721.
PPPD increases the risk of DGE than PrPD, especially SDGE. Our prediction nomogram gives good prediction of SDGE after pancreaticoduodenectomy.
胃排空延迟(DGE)是胰十二指肠切除术(PD)常见且令人困扰的并发症。研究表明手术方式及其他临床特征可能影响DGE的发生。然而,此类研究结果相互矛盾。本研究的目的是进行倾向评分匹配分析,以比较保留幽门胰十二指肠切除术(PPPD)和切除幽门胰十二指肠切除术(PrPD)之间的差异,并开发和验证一个列线图来预测严重胃排空延迟(SDGE)的概率。
这项回顾性研究纳入了2009年12月至2018年12月在我院接受PD的患者。采用1:1的比例进行倾向评分匹配,以比较PPPD组和PrPD组。我们比较了并发症发生率、DGE、住院时间、住院费用和死亡率。进行单因素和多因素逻辑回归分析以确定严重DGE的潜在危险因素。最后,开发并验证了一个列线图来预测严重DGE。
PPPD组术后胰瘘发生率显著更高(29.9%对17.4%,P<0.05),且失血量更少(463.7ml对694.9ml,P<0.05)。倾向评分匹配后,PPPD组术后DGE发生率显著高于PrPD组(19.2%对3.8%,P<0.05),尤其是严重DGE(17.3%对0%)。两组在住院时间、住院费用或死亡率方面无显著差异。手术方式、胆漏、腹腔感染和糖尿病是SDGE的独立危险因素。该列线图预测SDGE的训练C指数为0.798,验证C指数为0.721。
与PrPD相比,PPPD增加了DGE的风险,尤其是SDGE。我们的预测列线图对胰十二指肠切除术后的SDGE有良好的预测效果。