Roerden Malte, Nelde Annika, Heitmann Jonas S, Klein Reinhild, Rammensee Hans-Georg, Bethge Wolfgang A, Walz Juliane S
Department of Hematology, Oncology, Clinical Immunology and Rheumatology, University Hospital Tübingen, 72076 Tübingen, Germany.
Cluster of Excellence iFIT (EXC2180) "Image-Guided and Functionally Instructed Tumor Therapies", University of Tübingen, 72076 Tübingen, Germany.
Cancers (Basel). 2020 Jul 8;12(7):1835. doi: 10.3390/cancers12071835.
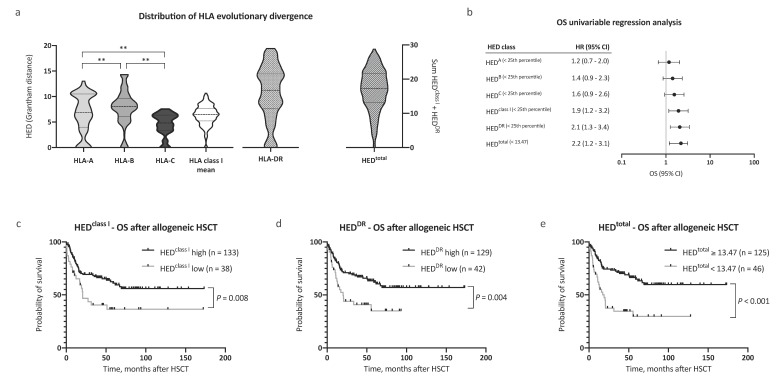
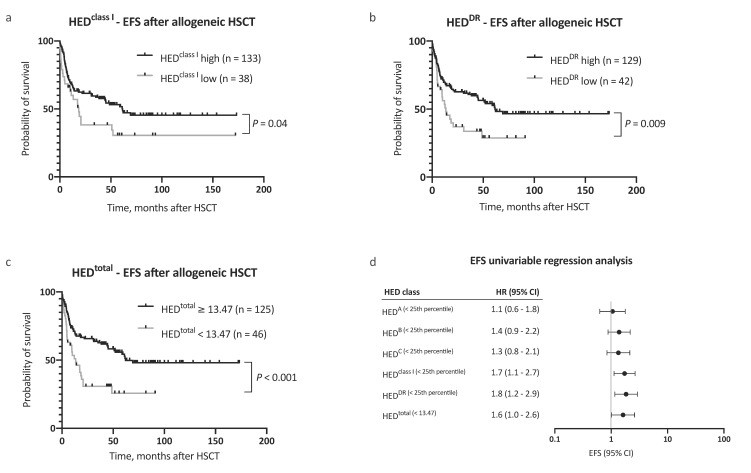
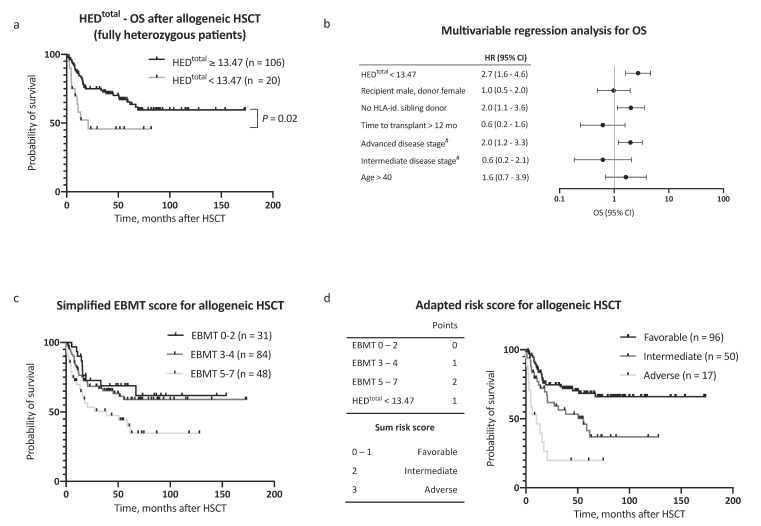
The diversity of human leukocyte antigens (HLAs) enables the presentation of immense repertoires of peptides, including tumor-associated antigens (TAAs). As a surrogate for immunopeptidome diversity, the HLA evolutionary divergence (HED) between individual HLA alleles might directly define the ability to present TAAs, a prerequisite for graft-versus-leukemia effects. We therefore analyzed the impact of HED on survival within a cohort of 171 acute myeloid leukemia (AML) patients after matched donor allogeneic hematopoietic stem cell transplantation (HSCT). Low HED (<25th percentile) of HLA class I (HED) or HLA-DR antigens (HED) was a strong determinant for adverse overall survival after allogeneic HSCT (OS), with a hazard ratio for death of 1.9 (95% CI 1.2-3.2) and 2.1 (95% CI 1.3-3.4), respectively. Defining a cutoff value for the combined HED (HED and HED), the respective 5 year OS was 29.7% and 64.9% in patients with low and high HED ( < 0.001), respectively. Furthermore, the risk of relapse was significantly higher in patients with low HED (hazard ratio (HR) 2.2, 95% CI 1.3-3.6) and event-free survival (EFS) was significantly reduced (5 year EFS 25.7% versus 54.4%, < 0.001). We here introduce HED, a fundamental metric of immunopeptidome diversity, as a novel prognostic factor for AML patients undergoing allogeneic HSCT.
人类白细胞抗原(HLA)的多样性使得包括肿瘤相关抗原(TAA)在内的大量肽段得以呈递。作为免疫肽组多样性的替代指标,个体HLA等位基因之间的HLA进化差异(HED)可能直接决定呈递TAA的能力,而这是移植物抗白血病效应的前提条件。因此,我们分析了HED对171例急性髓系白血病(AML)患者在匹配供体异基因造血干细胞移植(HSCT)后的生存影响。HLA I类抗原(HED)或HLA-DR抗原(HED)的低HED(<第25百分位数)是异基因HSCT后不良总生存(OS)的有力决定因素,死亡风险比分别为1.9(95%CI 1.2 - 3.2)和2.1(95%CI 1.3 - 3.4)。定义联合HED(HED和HED)的临界值,低HED和高HED患者(<0.001)的5年OS分别为29.7%和64.9%。此外,低HED患者的复发风险显著更高(风险比(HR)2.2,95%CI 1.3 - 3.6),无事件生存(EFS)显著降低(5年EFS为25.7%对54.4%,<0.001)。我们在此引入HED,这一免疫肽组多样性的基本指标,作为接受异基因HSCT的AML患者的一种新的预后因素。