Department of Medicine III (Interdisciplinary Medical Intensive Care), Medical Center-University of Freiburg, Faculty of Medicine, University of Freiburg, Hugstetter Straße 55, 79106, Freiburg, Germany.
Department of Cardiology and Angiology I, Heart Center Freiburg University, Faculty of Medicine, University of Freiburg, Freiburg, Germany.
J Thromb Thrombolysis. 2021 Feb;51(2):301-307. doi: 10.1007/s11239-020-02217-1.
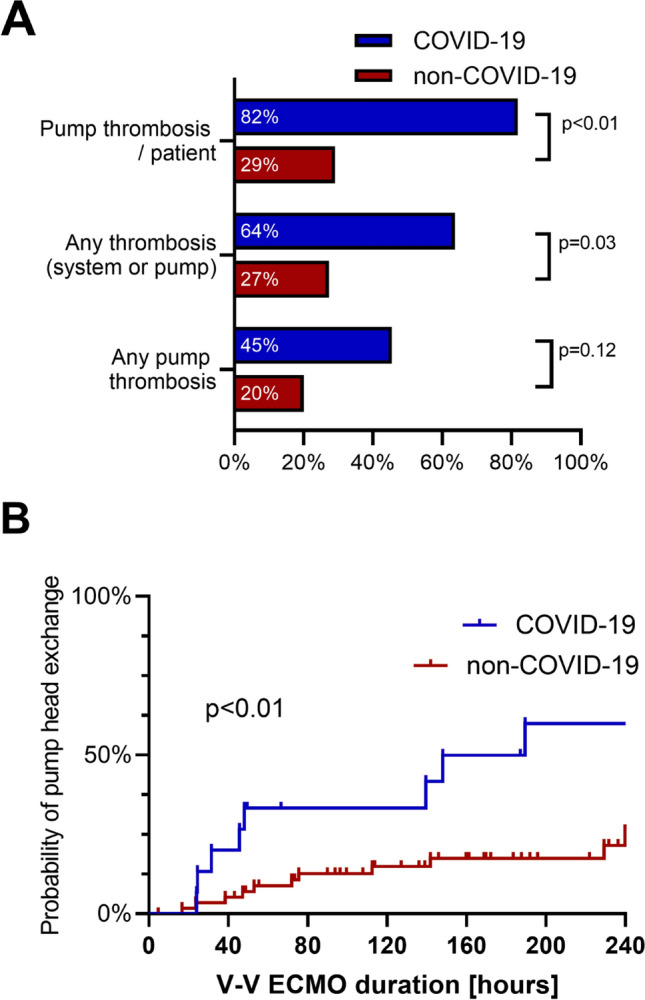
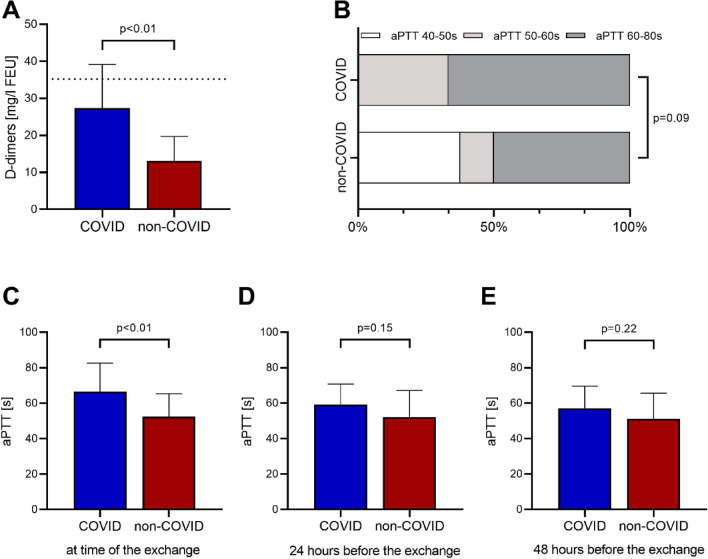
The novel coronavirus SARS-CoV-2 and the resulting disease COVID-19 causes pulmonary failure including severe courses requiring venovenous extracorporeal membrane oxygenation (V-V ECMO). Coagulopathy is a known complication of COVID-19 leading to thrombotic events including pulmonary embolism. It is unclear if the coagulopathy also increases thrombotic circuit complications of the ECMO. Aim of the present study therefor was to investigate the rate of V-V ECMO complications in COVID-19. We conducted a retrospective registry study including all patients on V-V ECMO treated at our centre between 01/2018 and 04/2020. COVID-19 cases were compared non- COVID-19 cases. All circuit related complications resulting in partial or complete exchange of the extracorporeal system were registered. In total, 66 patients were analysed of which 11 (16.7%) were SARS-CoV-2 positive. The two groups did not differ in clinical parameters including age (COVID-19 59.4 vs. non-COVID-19 58.1 years), gender (36.4% vs. 40%), BMI (27.8 vs. 24.2) and severity of illness as quantified by the RESP Score (1pt. vs 1pt.). 28 days survival was similar in both groups (72.7% vs. 58.2%). While anticoagulation was similar in both groups (p = 0.09), centrifugal pump head thrombosis was more frequent in COVID-19 (9/11 versus 16/55 p < 0.01). Neither the time to first exchange (p = 0.61) nor blood flow at exchange (p = 0.68) did differ in both groups. D-dimer levels prior to the thrombotic events were significantly higher in COVID-19 (mean 15.48 vs 26.59, p = 0.01). The SARS-CoV-2 induced infection is associated with higher rates of thrombotic events of the extracorporeal system during V-V ECMO therapy.
新型冠状病毒 SARS-CoV-2 及其引发的疾病 COVID-19 可导致包括需要静脉-静脉体外膜肺氧合(V-V ECMO)的严重病例在内的肺衰竭。凝血功能障碍是 COVID-19 的已知并发症,可导致包括肺栓塞在内的血栓事件。目前尚不清楚凝血功能障碍是否会增加 ECMO 的血栓性回路并发症。因此,本研究的目的是调查 COVID-19 患者 V-V ECMO 并发症的发生率。我们进行了一项回顾性登记研究,纳入了 2018 年 1 月至 2020 年 4 月期间在我院接受 V-V ECMO 治疗的所有患者。COVID-19 病例与非 COVID-19 病例进行了比较。所有与回路相关的并发症导致部分或完全更换体外系统的情况均进行了登记。共分析了 66 例患者,其中 11 例(16.7%)为 SARS-CoV-2 阳性。两组在临床参数方面无差异,包括年龄(COVID-19 59.4 岁 vs. 非 COVID-19 58.1 岁)、性别(36.4% vs. 40%)、BMI(27.8 与 24.2)和病情严重程度,由 RESP 评分(1 分 vs. 1 分)量化。两组 28 天存活率相似(72.7% vs. 58.2%)。两组抗凝治疗相似(p=0.09),但 COVID-19 组的离心泵头血栓形成更为常见(9/11 例 vs. 16/55 例,p<0.01)。两组首次更换的时间(p=0.61)和更换时的血流量(p=0.68)均无差异。COVID-19 患者血栓形成事件前 D-二聚体水平显著升高(平均值 15.48 与 26.59,p=0.01)。在 V-V ECMO 治疗期间,SARS-CoV-2 引起的感染与体外系统血栓形成事件的发生率较高有关。