Lubnow Matthias, Philipp Alois, Foltan Maik, Bull Enger Tone, Lunz Dirk, Bein Thomas, Haneya Assad, Schmid Christof, Riegger Günter, Müller Thomas, Lehle Karla
Department of Internal Medicine II, University Medical Center Regensburg, Franz-Josef-Strauss-Allee 11, 93042 Regensburg, Germany.
Department of Cardiothoracic Surgery, University Medical Center Regensburg, Franz-Josef-Strauss-Allee 11, 93042 Regensburg, Germany.
PLoS One. 2014 Dec 2;9(12):e112316. doi: 10.1371/journal.pone.0112316. eCollection 2014.
Technical complications are a known hazard in veno-venous extracorporeal membrane oxygenation (vvECMO). Identifying these complications and predictive factors indicating a developing system-exchange was the goal of the study.
Retrospective study on prospectively collected data of technical complications including 265 adult patients (Regensburg ECMO Registry, 2009-2013) with acute respiratory failure treated with vvECMO. Alterations in blood flow resistance, gas transfer capability, hemolysis, coagulation and hemostasis parameters were evaluated in conjunction with a system-exchange in all patients with at least one exchange (n = 83).
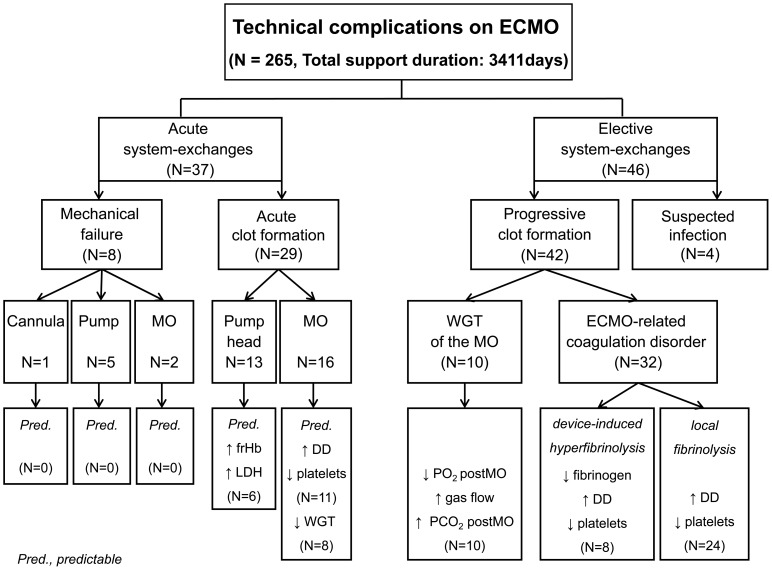
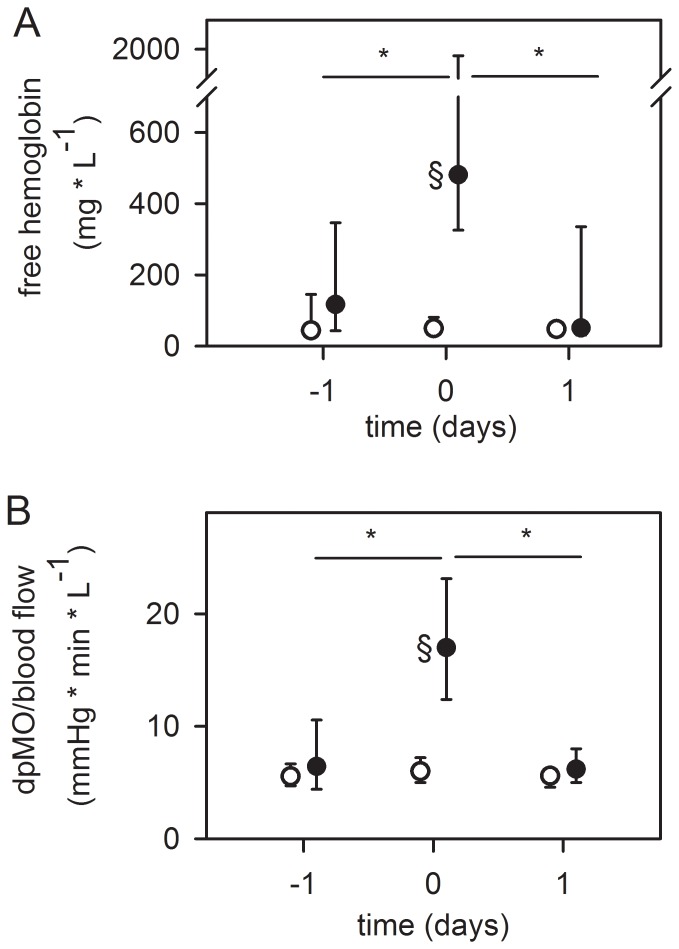
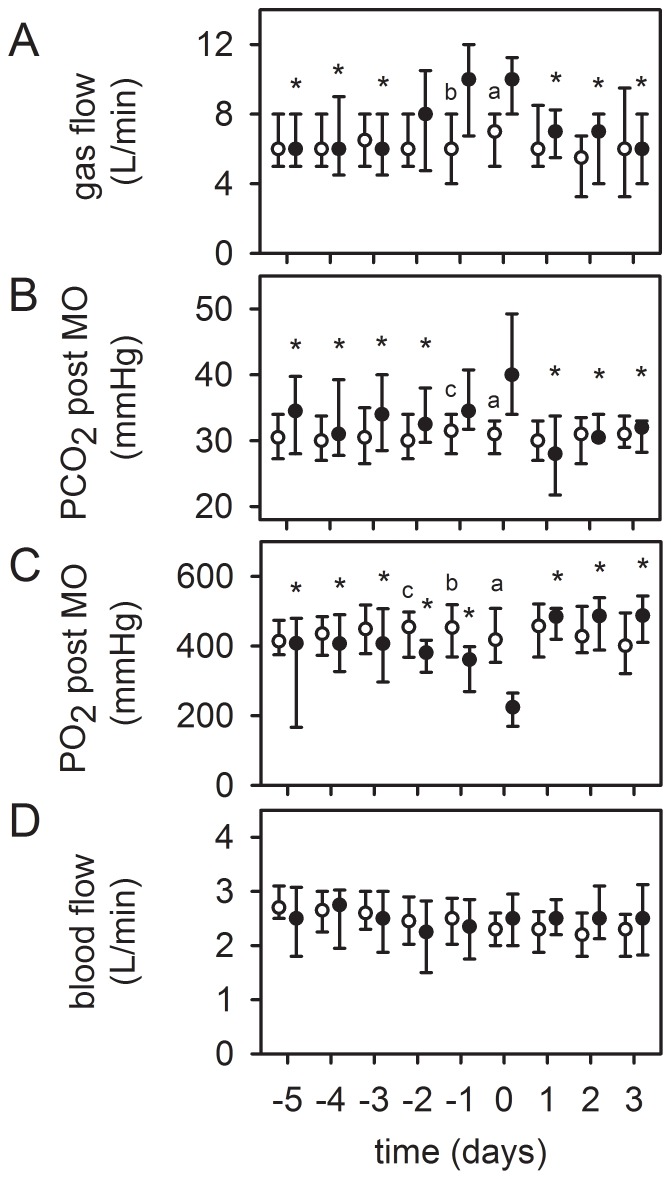
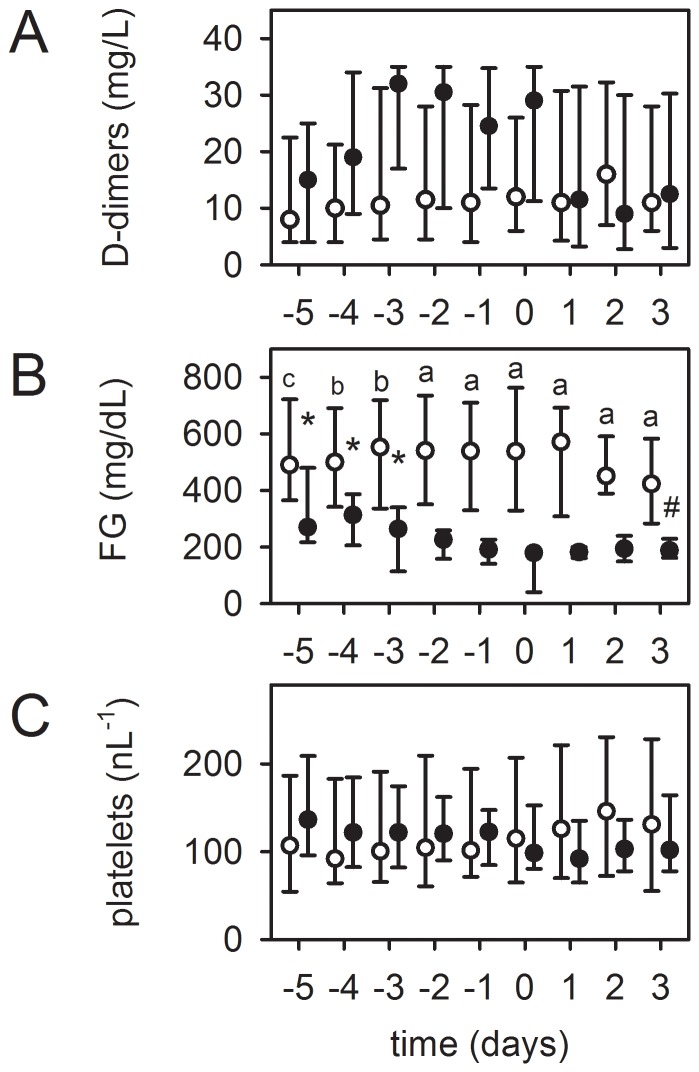
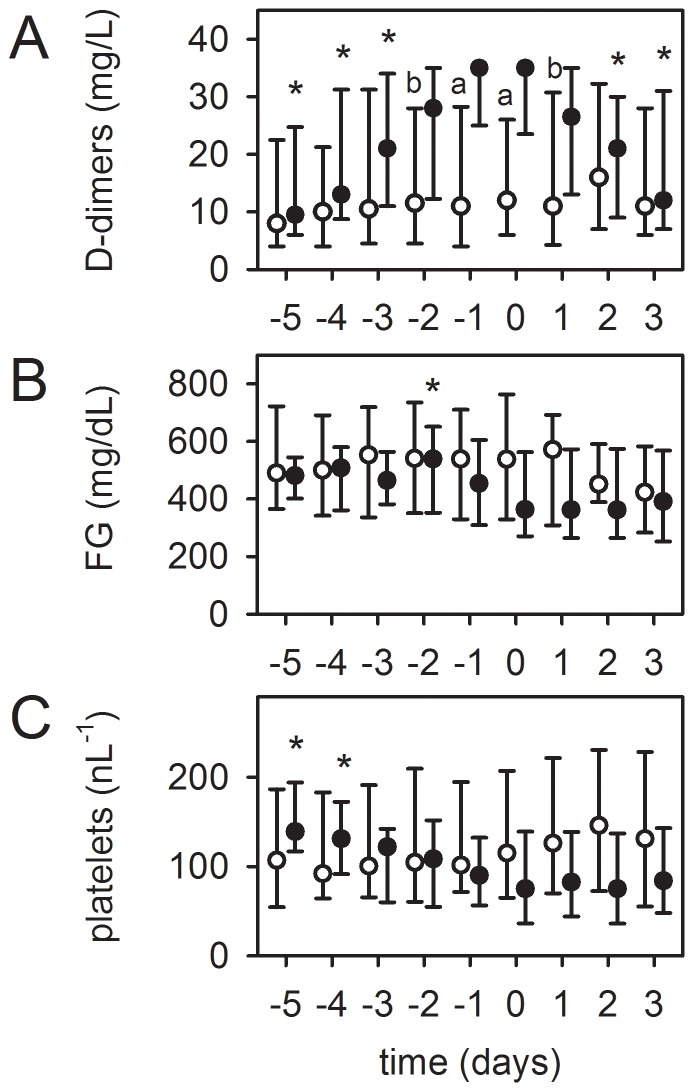
Values presented as median (interquartile range). Patient age was 50(36-60) years, the SOFA score 11(8-14.3) and the Murray lung injury Score 3.33(3.3-3.7). Cumulative ECMO support time 3411 days, 9(6-15) days per patient. Mechanical failure of the blood pump (n = 5), MO (n = 2) or cannula (n = 1) accounted for 10% of the exchanges. Acute clot formation within the pump head (visible clots, increase in plasma free hemoglobin (frHb), serum lactate dehydrogenase (LDH), n = 13) and MO (increase in pressure drop across the MO, n = 16) required an urgent system-exchange, of which nearly 50% could be foreseen by measuring the parameters mentioned below. Reasons for an elective system-exchange were worsening of gas transfer capability (n = 10) and device-related coagulation disorders (n = 32), either local fibrinolysis in the MO due to clot formation (increased D-dimers [DD]), decreased platelet count; n = 24), or device-induced hyperfibrinolysis (increased DD, decreased fibrinogen [FG], decreased platelet count, diffuse bleeding tendency; n = 8), which could be reversed after system-exchange. Four MOs were exchanged due to suspicion of infection.
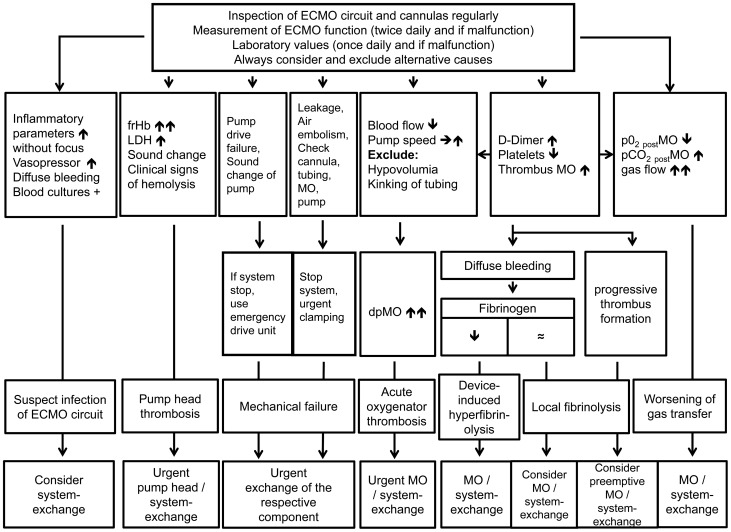
The majority of ECMO system-exchanges could be predicted by regular inspection of the complete ECMO circuit, evaluation of gas exchange, pressure drop across the MO and laboratory parameters (DD, FG, platelets, LDH, frHb). These parameters should be monitored in the daily routine to reduce the risk of unexpected ECMO failure.
技术并发症是静脉 - 静脉体外膜肺氧合(vvECMO)中已知的风险。识别这些并发症以及表明系统即将更换的预测因素是本研究的目标。
对前瞻性收集的包括265例接受vvECMO治疗的急性呼吸衰竭成年患者(雷根斯堡ECMO登记处,2009 - 2013年)的技术并发症数据进行回顾性研究。对所有至少进行过一次系统更换(n = 83)的患者,评估血流阻力、气体交换能力、溶血、凝血和止血参数的变化,并与系统更换情况相结合进行分析。
数据以中位数(四分位间距)表示。患者年龄为50(36 - 60)岁,序贯器官衰竭评估(SOFA)评分1l(8 - 14.3),默里肺损伤评分3.33(3.3 - 3.7)。ECMO累计支持时间为3411天,每位患者9(6 - 15)天。血泵机械故障(n = 5)、膜氧合器(MO)故障(n = 2)或插管故障(n = 1)占系统更换的10%。泵头内急性血栓形成(可见血栓、血浆游离血红蛋白(frHb)升高、血清乳酸脱氢酶(LDH)升高,n = 13)和MO故障(MO两端压降升高,n = 16)需要紧急更换系统,其中近50%可通过测量下述参数预见。择期更换系统的原因是气体交换能力恶化(n = 10)和与设备相关的凝血障碍(n = 32),后者包括因血栓形成导致MO局部纤溶(D - 二聚体[DD]升高)、血小板计数降低(n = 24),或设备诱导的高纤溶状态(DD升高、纤维蛋白原[FG]降低、血小板计数降低、弥漫性出血倾向,n = 8),系统更换后这些情况可逆转。4个MO因怀疑感染而更换。
通过定期检查完整的ECMO回路、评估气体交换、MO两端压降以及实验室参数(DD、FG、血小板、LDH、frHb),大多数ECMO系统更换情况可被预测。日常应监测这些参数,以降低ECMO意外故障的风险。