Division of Gastroenterology and Hepatology, Department of Internal Medicine III, Medical University of Vienna, Vienna, Austria.
Vienna Hepatic Hemodynamic Laboratory, Medical University of Vienna, Vienna, Austria.
Hepatology. 2021 Apr;73(4):1275-1289. doi: 10.1002/hep.31462. Epub 2021 Mar 16.
Risk stratification after cure from hepatitis C virus (HCV) infection remains a clinical challenge. We investigated the predictive value of noninvasive surrogates of portal hypertension (liver stiffness measurement [LSM] by vibration-controlled transient elastography and von Willebrand factor/platelet count ratio [VITRO]) for development of hepatic decompensation and hepatocellular carcinoma in patients with pretreatment advanced chronic liver disease (ACLD) who achieved HCV cure.
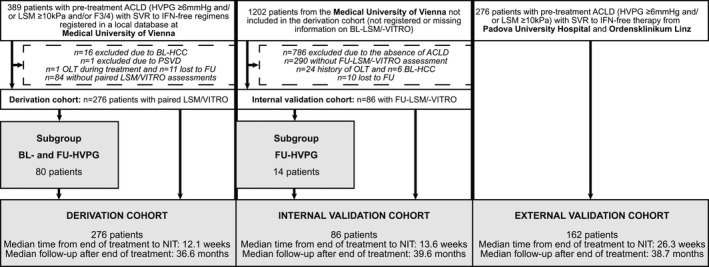
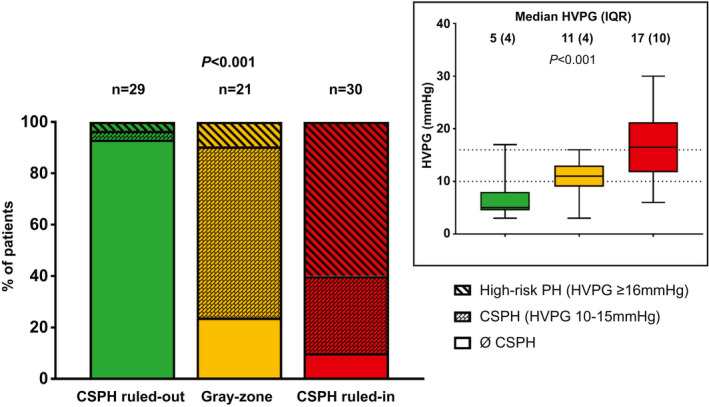
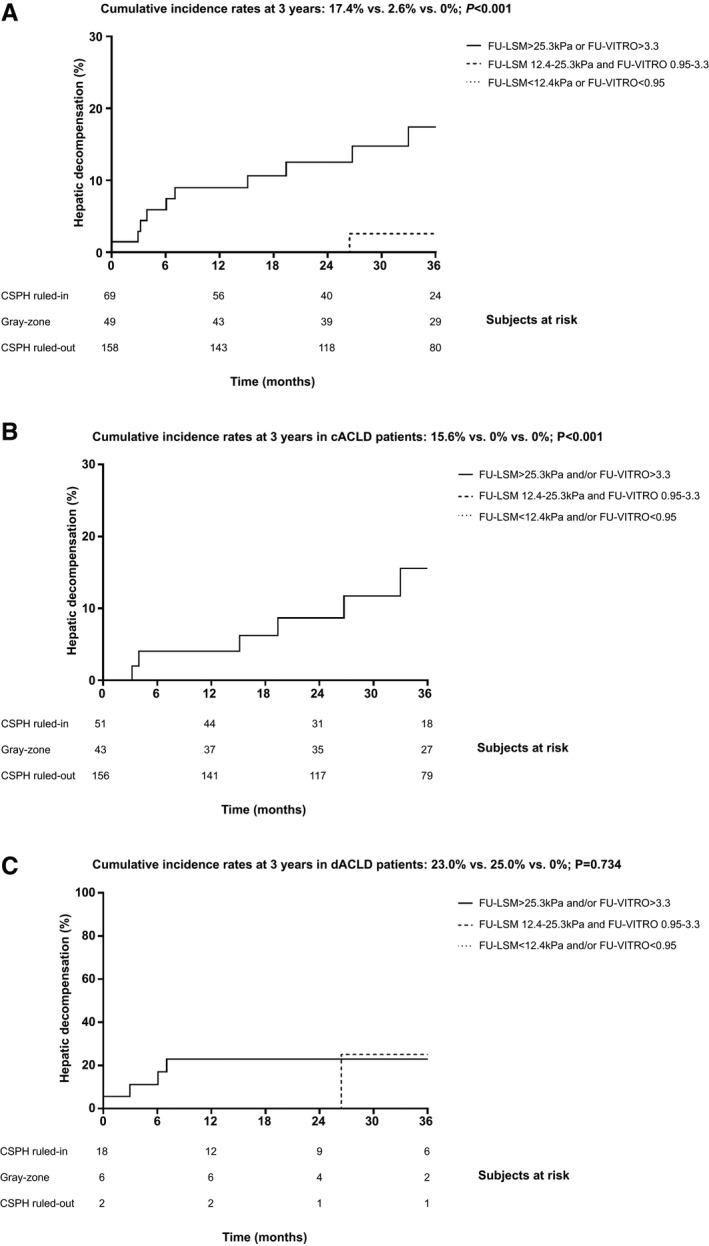
A total of 276 patients with pretreatment ACLD and information on pretreatment and posttreatment follow-up (FU)-LSM and FU-VITRO were followed for a median of 36.6 months after the end of interferon-free therapy. FU-LSM (area under the receiver operating characteristic curve [AUROC]: 0.875 [95% confidence interval [CI]: 0.796-0.954]) and FU-VITRO (AUROC: 0.925 [95% CI: 0.874-0.977]) showed an excellent predictive performance for hepatic decompensation. Both parameters provided incremental information and were significantly associated with hepatic decompensation in adjusted models. A previously proposed combined approach (FU-LSM < 12.4 kPa and/or FU-VITRO < 0.95) to rule out clinically significant portal hypertension (CSPH, hepatic venous pressure gradient ≥10 mm Hg) at FU assigned most (57.3%) of the patients to the low-risk group; none of these patients developed hepatic decompensation. In contrast, in patients in whom FU-CSPH was ruled in (FU-LSM > 25.3 kPa and/or FU-VITRO > 3.3; 25.0% of patients), the risk of hepatic decompensation at 3 years following treatment was high (17.4%). Patients within the diagnostic gray-zone for FU-CSPH (17.8% of patients) had a very low risk of hepatic decompensation during FU (2.6%). The prognostic value of this algorithm was validated in an internal (n = 86) and external (n = 162) cohort.
FU-LSM/FU-VITRO are strongly and independently predictive of posttreatment hepatic decompensation in HCV-induced ACLD. An algorithm combining these noninvasive markers not only rules in or rules out FU-CSPH, but also identifies populations at negligible versus high risk for hepatic decompensation. FU-LSM/FU-VITRO are readily accessible and enable risk stratification after sustained virological response, and thus facilitate personalized management.
丙型肝炎病毒(HCV)感染治愈后,风险分层仍然是一个临床挑战。我们研究了非侵入性门脉高压替代标志物(振动控制瞬态弹性成像的肝硬度测量[LSM]和血管性血友病因子/血小板计数比值[VITRO])对治疗前进展性慢性肝病(ACLD)患者发生肝失代偿和肝细胞癌的预测价值,这些患者在无干扰素治疗结束后进行了治疗。
共有 276 名治疗前 ACLD 患者,我们对其进行了治疗前和治疗后随访(FU)-LSM 和 FU-VITRO 的信息随访,平均随访 36.6 个月。FU-LSM(接受者操作特征曲线下面积[AUC]:0.875[95%置信区间[CI]:0.796-0.954])和 FU-VITRO(AUC:0.925[95%CI:0.874-0.977])对肝失代偿有很好的预测作用。这两个参数都提供了附加信息,并在调整后的模型中与肝失代偿显著相关。一个之前提出的用于排除 FU 时临床显著门脉高压(CSPH,肝静脉压力梯度≥10mmHg)的联合方法(FU-LSM<12.4kPa 和/或 FU-VITRO<0.95)将大多数(57.3%)患者分配到低风险组;这些患者中无一例发生肝失代偿。相比之下,在 FU-CSPH 被判定为阳性的患者(FU-LSM>25.3kPa 和/或 FU-VITRO>3.3;占患者的 25.0%)中,治疗后 3 年肝失代偿的风险很高(17.4%)。FU-CSPH 诊断灰色地带的患者(占患者的 17.8%)在 FU 期间肝失代偿的风险非常低(2.6%)。该算法的预后价值在内部(n=86)和外部(n=162)队列中得到了验证。
FU-LSM/FU-VITRO 可强烈且独立地预测 HCV 诱导的 ACLD 患者治疗后的肝失代偿。该算法不仅可以用于确定或排除 FU-CSPH,还可以识别出发生肝失代偿的低风险和高风险人群。FU-LSM/FU-VITRO 易于获得,并可在持续病毒学应答后进行风险分层,从而有助于实现个体化管理。