Kurihara Toru, Igarashi Yutaka, Kobai Kaori, Mizobuchi Taiki, Ishii Hiromoto, Matsumoto Noriko, Yokobori Shoji, Yokota Hiroyuki
Department of Emergency and Critical Care Medicine Nippon Medical School Hospital Tokyo Japan.
Department of Anesthesiology Wakayama Medical University Wakayama Japan.
Acute Med Surg. 2020 Jun 2;7(1):e517. doi: 10.1002/ams2.517. eCollection 2020 Jan-Dec.
It is difficult to diagnose Bickerstaff's brainstem encephalitis (BBE) in the acute phase, and emergency physicians could diagnose BBE as an unknown cause of consciousness disturbance.
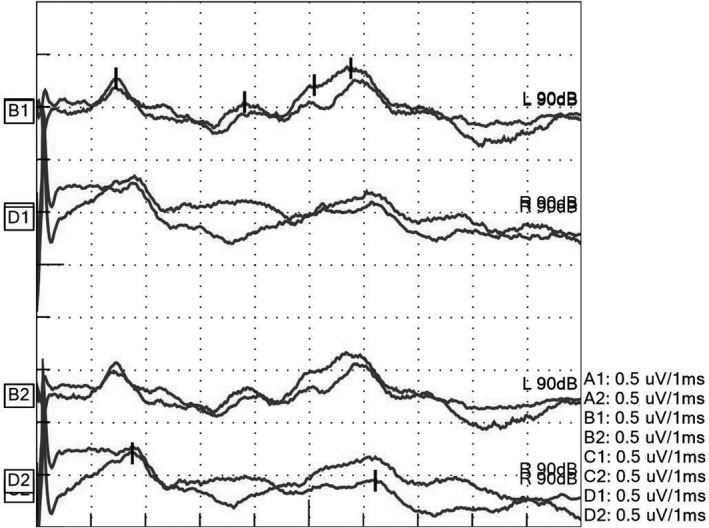
A 75-year-old woman presented with dizziness and weakness in both arms 1 week after an upper respiratory infection. She experienced gradual worsening of consciousness, had dilated pupils and no light reflex. She was suspected of brainstem dysfunction at the upper part of the brainstem; however, there were not significant findings on magnetic resonance imaging, cerebrospinal fluid, or electroencephalography. The auditory brainstem response demonstrated a low voltage, but there was no prolonged latency. At a later date, she was diagnosed with BBE based on serum immunoglobulin G anti-GQ1b antibody. She was discharged home without any neurological sequelae.
It is necessary to analyze serum immunoglobulin G anti-GQ1b antibodies to diagnose BBE. Auditory brainstem response would be helpful in detecting lesions and predicting functional recovery.
在急性期很难诊断出比克斯特法脑干脑炎(BBE),急诊医生可能会将BBE诊断为意识障碍的不明原因。
一名75岁女性在上呼吸道感染1周后出现头晕和双臂无力。她的意识逐渐恶化,瞳孔散大且无光反射。怀疑她脑干上部存在功能障碍;然而,磁共振成像、脑脊液或脑电图检查均未发现明显异常。听觉脑干反应显示电压低,但潜伏期未延长。后来,根据血清免疫球蛋白G抗GQ1b抗体诊断她患有BBE。她出院时没有任何神经后遗症。
分析血清免疫球蛋白G抗GQ1b抗体对于诊断BBE很有必要。听觉脑干反应有助于检测病变并预测功能恢复。