Deliwala Smit S, Ponnapalli Anoosha, Seedahmed Elfateh, Berrou Mohammed, Bachuwa Ghassan, Chandran Arul
Department of Internal Medicine, Michigan State University at Hurley Medical Center, Flint, MI, USA.
Department of Internal Medicine - Division of Pulmonology/Critical Care, Michigan State University at Hurley Medical Center, Flint, MI, USA.
Am J Case Rep. 2020 Jul 23;21:e926136. doi: 10.12659/AJCR.926136.
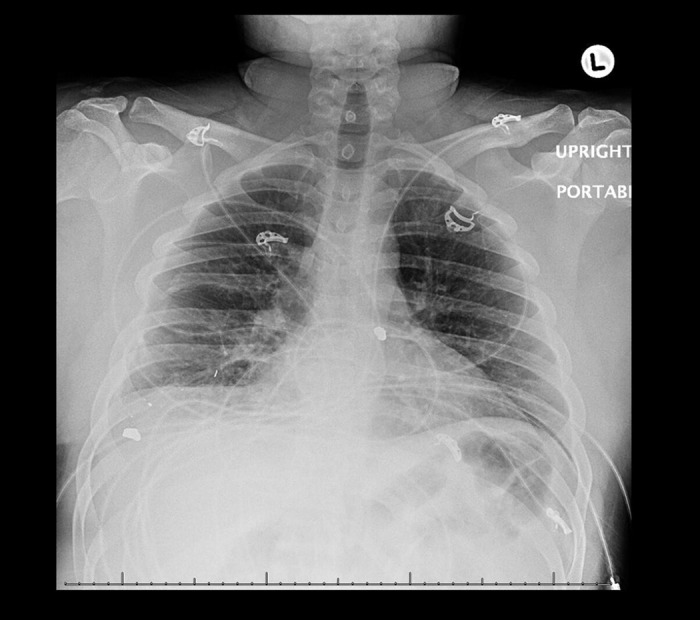
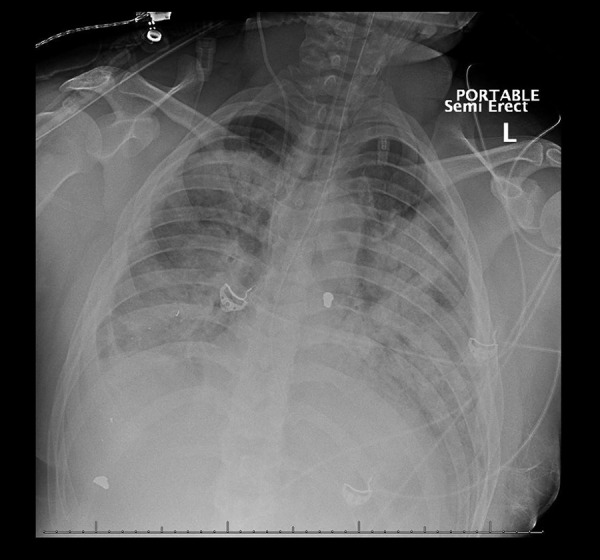
BACKGROUND COVID-19 patients that develop acute respiratory distress syndrome (ARDS) "CARDS" behave differently compared to patients with classic forms of ARDS. Recently 2 CARDS phenotypes have been described, Type L and Type H. Most patients stabilize at the milder form, Type L, while an unknown subset progress to Type H, resembling full-blown ARDS. If uncorrected, phenotypic conversion can induce a rapid downward spiral towards progressive lung injury, vasoplegia, and pulmonary shrinkage, risking ventilator-induced lung injury (VILI) known as the "VILI vortex". No cases of in-hospital phenotypic conversion have been reported, while ventilation strategies in these patients differ from the lung-protective approaches seen in classic ARDS. CASE REPORT A 29-year old male was admitted with COVID-19 pneumonia complicated by severe ARDS, multi-organ failure, cytokine release syndrome, and coagulopathy during his admission. He initially resembled CARDS Type L case, although refractory hypoxemia, fevers, and a high viral burden prompted conversion to Type H within 8 days. Despite ventilation strategies, neuromuscular blockade, inhalation therapy, and vitamin C, he remained asynchronous to the ventilator with volumes and pressures beyond accepted thresholds, eventually developing a fatal tension pneumothorax. CONCLUSIONS Patients that convert to Type H can quickly enter a spiral of hypoxemia, shunting, and dead-space ventilation towards full-blown ARDS. Understanding its nuances is vital to interrupting phenotypic conversion and entry into VILI vortex. Tension pneumothorax represents a poor outcome in patients with CARDS. Further research into monitoring lung dynamics, modifying ventilation strategies, and understanding response to various modes of ventilation in CARDS are required to mitigate these adverse outcomes.
与患有经典形式急性呼吸窘迫综合征(ARDS)的患者相比,发展为急性呼吸窘迫综合征(“CARDS”)的新型冠状病毒肺炎(COVID-19)患者表现不同。最近描述了2种CARDS表型,即L型和H型。大多数患者病情稳定在较轻的L型,而有一部分未知患者会进展为H型,类似于典型的ARDS。如果不加以纠正,表型转换会导致病情迅速恶化,发展为进行性肺损伤、血管麻痹和肺萎陷,有发生呼吸机诱导性肺损伤(VILI)即“VILI漩涡”的风险。目前尚未报告院内表型转换的病例,而这些患者的通气策略与经典ARDS的肺保护性方法不同。病例报告:一名29岁男性因COVID-19肺炎入院,住院期间并发严重ARDS、多器官功能衰竭、细胞因子释放综合征和凝血病。他最初类似CARDS的L型病例,尽管难治性低氧血症、发热和高病毒载量促使其在8天内转换为H型。尽管采取了通气策略、神经肌肉阻滞、吸入治疗和维生素C治疗,他仍与呼吸机不同步,潮气量和压力超出可接受阈值,最终发展为致命的张力性气胸。结论:转换为H型的患者可迅速进入低氧血症、分流和无效腔通气的恶性循环,发展为典型的ARDS。了解其细微差别对于中断表型转换和进入VILI漩涡至关重要。张力性气胸是CARDS患者的不良结局。需要进一步研究监测CARDS患者的肺动力学、调整通气策略以及了解对各种通气模式的反应,以减轻这些不良后果。