Foundation for Clinical and Applied Cancer Research (FICMAC), Bogotá, Colombia.
Molecular Oncology and Biology Systems Research Group (FOX-G), Universidad el Bosque, Bogotá, Colombia.
Thorac Cancer. 2020 Sep;11(9):2552-2560. doi: 10.1111/1759-7714.13573. Epub 2020 Jul 24.
The intestinal microbiota is an important factor in modulating immune-mediated tumor cell destruction. Alterations in the microbiome composition have been linked to reduced efficacy of immune checkpoint inhibitor (ICI) therapies. Therefore, antibiotic treatment (ATB), which modifies the diversity of the gut bacteria populations, could lead to a reduced efficacy of ICI treatments.
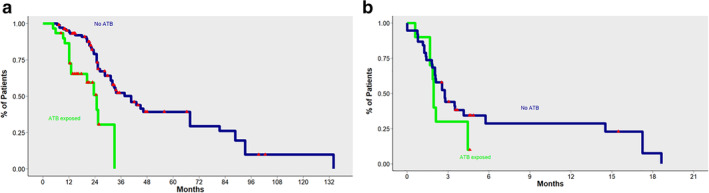
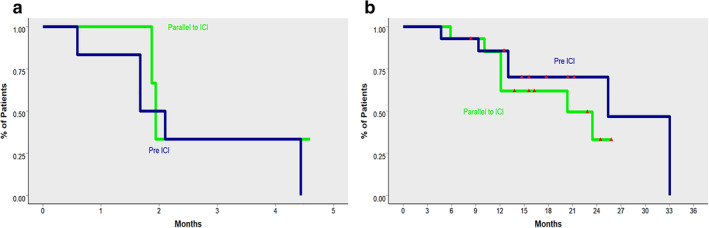
This was a retrospective cohort study. Patients with advanced non-small cell lung cancer (NSCLC) treated with anti-programmed cell death ligand-1 (PD-L1) alone, or in combination in three different countries in Latin America were included. After identification, patients were placed into three groups: Non-ATB exposed (no-ATB), exposed within 30 days of the first dose of ICI (pre-ICI ATB) and patients receiving ATB concomitantly with ICI (ICI-ATB). Progression-free survival (PFS), overall survival (OS) and response rates to treatment with ICI were assessed.
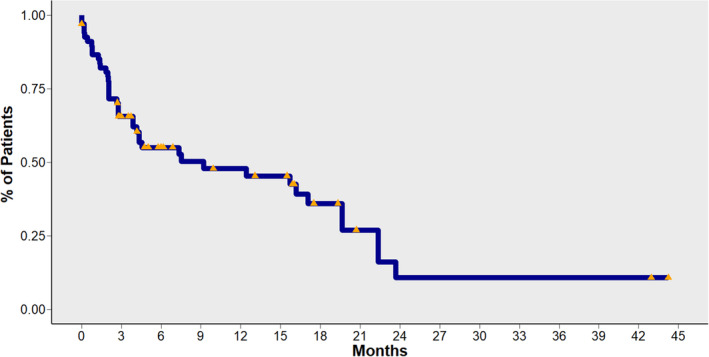
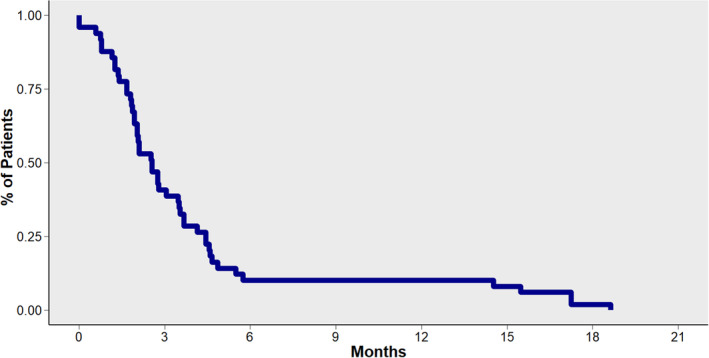
A total of 140 patients were included, of which 32 patients (23%) received ATB treatment. The most common ATB types were fluoroquinolones and B-lactams. No differences in survival according to antibiotic type were identified. Median OS in patients not exposed to ATB was 40.6 months (95% CI: 32-67.7), compared with 20.3 months (95% CI: 12.1-non-reached [NR]) for patients with pre-ICI ATB treatment and 24.7 months (95% CI: 13-NR) for patients treated with ATB concomitantly with ICI. There were no significant differences in terms of PFS, or response rates across all treatment groups.
Antibiotic treatment was associated with reduced OS in Hispanic patients with NSCLC treated with ICIs.
肠道微生物群是调节免疫介导的肿瘤细胞破坏的一个重要因素。微生物群组成的改变与免疫检查点抑制剂(ICI)治疗效果降低有关。因此,抗生素治疗(ATB)改变了肠道细菌种群的多样性,可能导致 ICI 治疗效果降低。
这是一项回顾性队列研究。纳入了在拉丁美洲三个国家接受单独或联合抗程序性死亡配体-1(PD-L1)治疗的晚期非小细胞肺癌(NSCLC)患者。识别后,患者被分为三组:未暴露于 ATB(无 ATB)组、ICI 治疗前 30 天内暴露于 ATB(ICI 前 ATB)组和同时接受 ATB 与 ICI 治疗(ICI-ATB)组。评估无进展生存期(PFS)、总生存期(OS)和对 ICI 治疗的反应率。
共纳入 140 例患者,其中 32 例(23%)接受了 ATB 治疗。最常见的 ATB 类型是氟喹诺酮类和β-内酰胺类。根据抗生素类型,未发现生存差异。未暴露于 ATB 的患者中位 OS 为 40.6 个月(95%CI:32-67.7),ICI 前 ATB 治疗患者为 20.3 个月(95%CI:12.1-NR),同时接受 ATB 与 ICI 治疗的患者为 24.7 个月(95%CI:13-NR)。在所有治疗组中,PFS 或反应率均无显著差异。
在接受 ICI 治疗的西班牙裔 NSCLC 患者中,抗生素治疗与 OS 降低相关。