Ikizler T Alp, Parikh Chirag R, Himmelfarb Jonathan, Chinchilli Vernon M, Liu Kathleen D, Coca Steven G, Garg Amit X, Hsu Chi-Yuan, Siew Edward D, Wurfel Mark M, Ware Lorraine B, Faulkner Georgia Brown, Tan Thida C, Kaufman James S, Kimmel Paul L, Go Alan S
Division of Nephrology and Hypertension, Vanderbilt University Medical Center, Nashville, Tennessee, USA.
Division of Nephrology, Department of Medicine, Johns Hopkins School of Medicine, Baltimore, Maryland, USA.
Kidney Int. 2021 Feb;99(2):456-465. doi: 10.1016/j.kint.2020.06.032. Epub 2020 Jul 22.
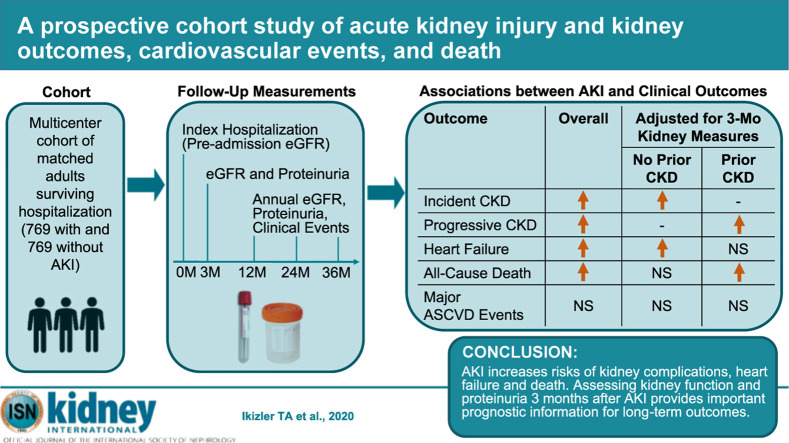
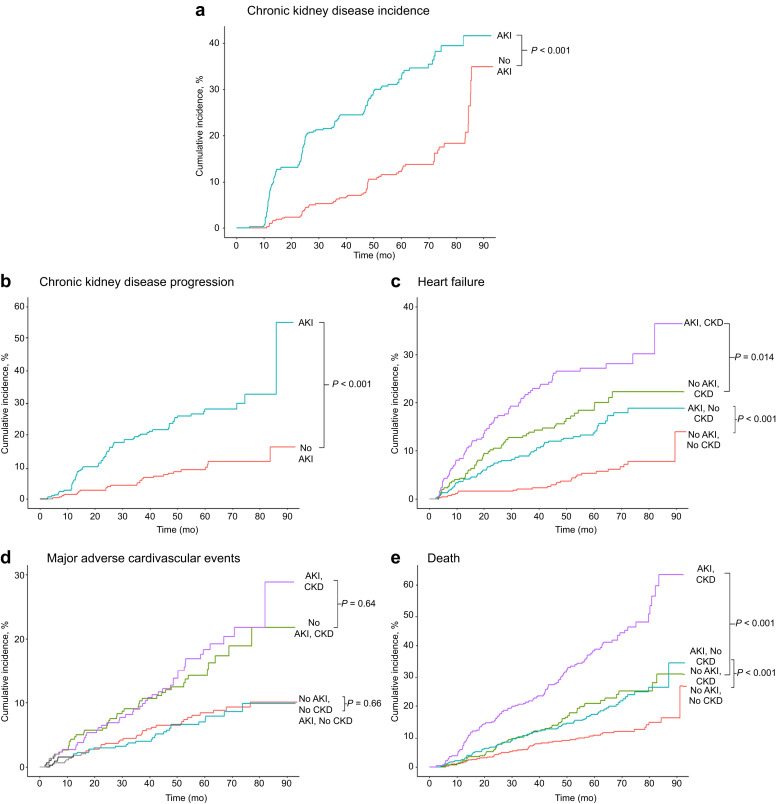
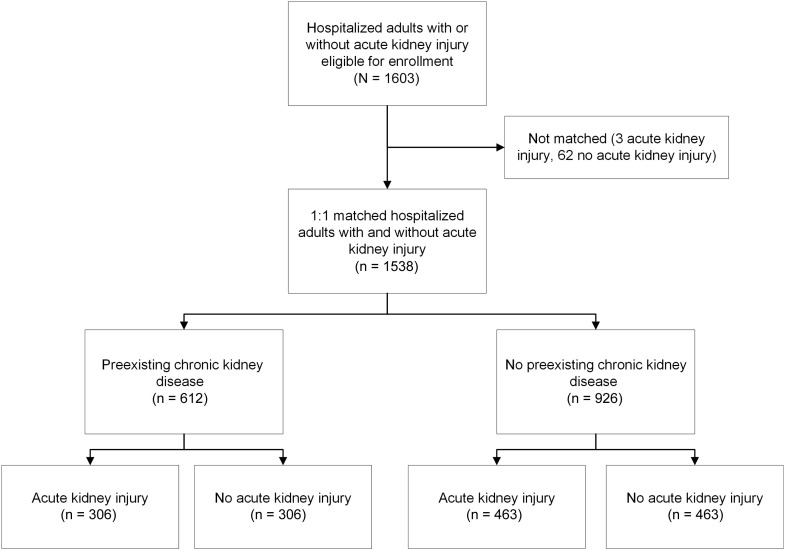
Acute kidney injury (AKI) has been reported to be associated with excess risks of death, kidney disease progression and cardiovascular events although previous studies have important limitations. To further examine this, we prospectively studied adults from four clinical centers surviving three months and more after hospitalization with or without AKI who were matched on center, pre-admission CKD status, and an integrated priority score based on age, prior cardiovascular disease or diabetes mellitus, preadmission estimated glomerular filtration rate (eGFR) and treatment in the intensive care unit during the index hospitalization between December 2009-February 2015, with follow-up through November 2018. All participants had assessments of kidney function before (eGFR) and at three months and annually (eGFR and proteinuria) after the index hospitalization. Associations of AKI with outcomes were examined after accounting for pre-admission and three-month post-discharge factors. Among 769 AKI (73% Stage 1, 14% Stage 2, 13% Stage 3) and 769 matched non-AKI adults, AKI was associated with higher adjusted rates of incident CKD (adjusted hazard ratio 3.98, 95% confidence interval 2.51-6.31), CKD progression (2.37,1.28-4.39), heart failure events (1.68, 1.22-2.31) and all-cause death (1.78, 1.24-2.56). AKI was not associated with major atherosclerotic cardiovascular events in multivariable analysis (0.95, 0.70-1.28). After accounting for degree of kidney function recovery and proteinuria at three months after discharge, the associations of AKI with heart failure (1.13, 0.80-1.61) and death (1.29, 0.84-1.98) were attenuated and no longer significant. Thus, assessing kidney function recovery and proteinuria status three months after AKI provides important prognostic information for long-term clinical outcomes.
据报道,急性肾损伤(AKI)与死亡、肾病进展和心血管事件的额外风险相关,尽管先前的研究存在重要局限性。为了进一步研究这一问题,我们对来自四个临床中心的成年人进行了前瞻性研究,这些成年人在2009年12月至2015年2月期间因有或无AKI住院后存活三个月及以上,根据中心、入院前慢性肾脏病(CKD)状态以及基于年龄、既往心血管疾病或糖尿病、入院前估计肾小球滤过率(eGFR)和指数住院期间在重症监护病房的治疗情况进行匹配,并随访至2018年11月。所有参与者在指数住院前(eGFR)以及住院后三个月和每年(eGFR和蛋白尿)均进行肾功能评估。在考虑入院前和出院后三个月的因素后,研究了AKI与结局的关联。在769例AKI患者(73%为1期,14%为2期,13%为3期)和769例匹配的非AKI成年人中,AKI与更高的CKD发病率调整率(调整后风险比3.98,95%置信区间2.51 - 6.31)、CKD进展(2.37,1.28 - 4.39)、心力衰竭事件(1.68,1.22 - 2.31)和全因死亡(1.78,1.24 - 2.56)相关。在多变量分析中,AKI与主要动脉粥样硬化性心血管事件无关(0.95,0.70 - 1.28)。在考虑出院后三个月的肾功能恢复程度和蛋白尿情况后,AKI与心力衰竭(1.13,0.80 - 1.61)和死亡(1.29,0.84 - 1.98)的关联减弱且不再显著。因此,评估AKI三个月后的肾功能恢复和蛋白尿状态可为长期临床结局提供重要的预后信息。