Population Health and Immunity Division, Walter and Eliza Hall Institute of Medical Research, Melbourne, VIC, Australia; Department of Medical Biology, University of Melbourne, Melbourne, VIC, Australia; Diagnostic Haematology, The Royal Melbourne Hospital, and Clinical Haematology at The Peter MacCallum Cancer Centre and The Royal Melbourne Hospital, Melbourne, VIC, Australia.
Global Health and Development, Department of Infectious Disease Epidemiology, Imperial College London, London, UK.
Lancet Glob Health. 2020 Aug;8(8):e1071-e1080. doi: 10.1016/S2214-109X(20)30240-0.
Universal home fortification of complementary foods with iron-containing multiple micronutrient powders (MNPs) is a key intervention to prevent anaemia in young children in low-income and middle-income countries. However, evidence that MNPs might promote infection raises uncertainty about whether MNPs give net health benefits and are cost-effective. We aimed to determined country-specific net benefit or harm and cost-effectiveness of universal provision of MNPs to children aged 6 months.
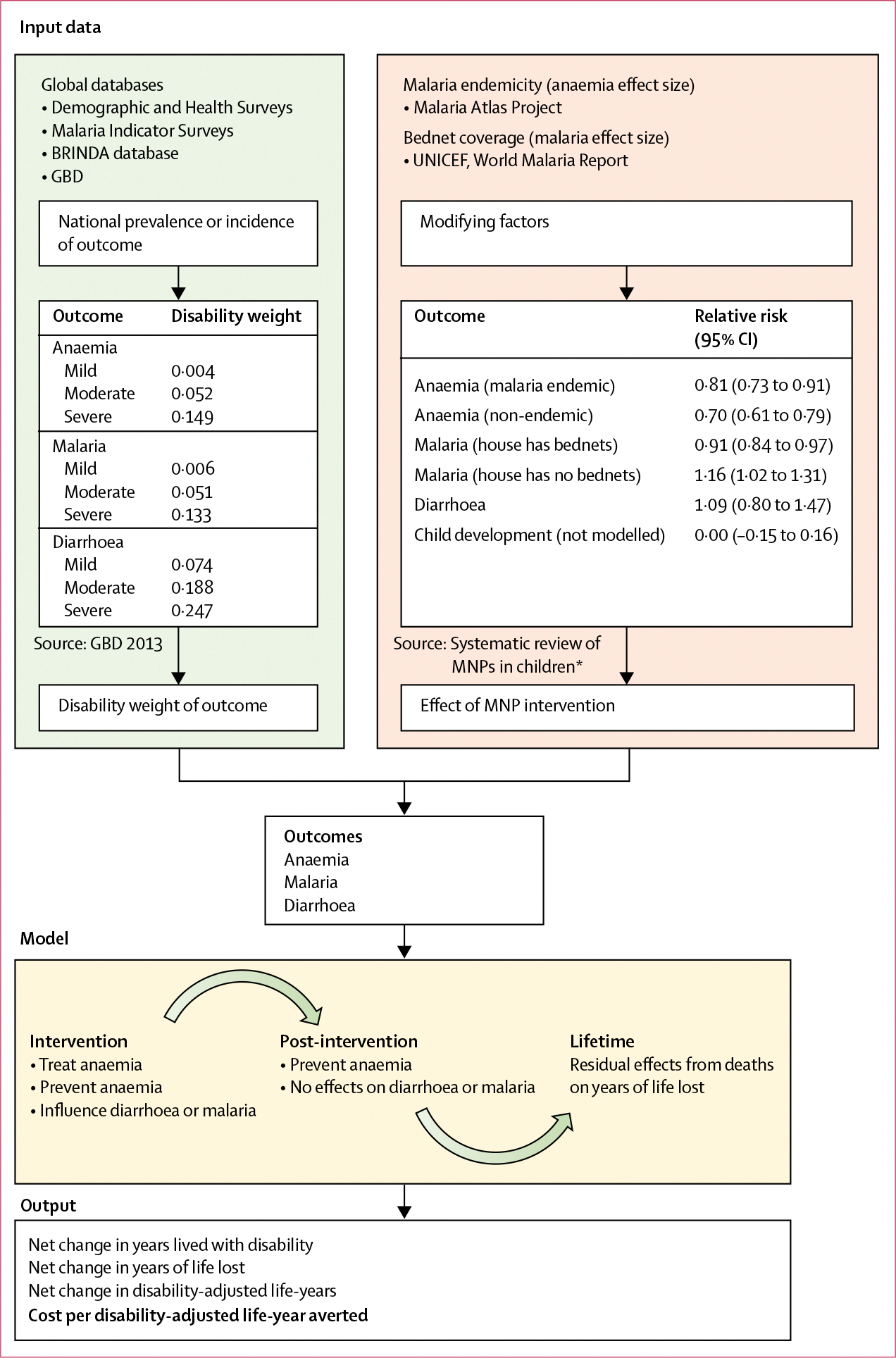
We developed a microsimulation model to estimate net country-specific disability-adjusted life-years (DALYs), years lived with disability (YLDs), and years of life lost (YLLs) due to anaemia, malaria, and diarrhoea averted (or increased) by provision of a 6-month course of MNPs to children aged 6 months, compared with no intervention, who would be followed up for an additional 6 months (ie, to age 18 months). Anaemia prevalence was derived from Demographic and Health Surveys or similar national surveys, and malaria and diarrhoea incidence were sourced from the Global Burden of Disease Study. Programme and health-care costs were modelled to determine cost per DALY averted (US$). Additionally, we explored the effects of reduced MNP coverage in a sensitivity analysis.
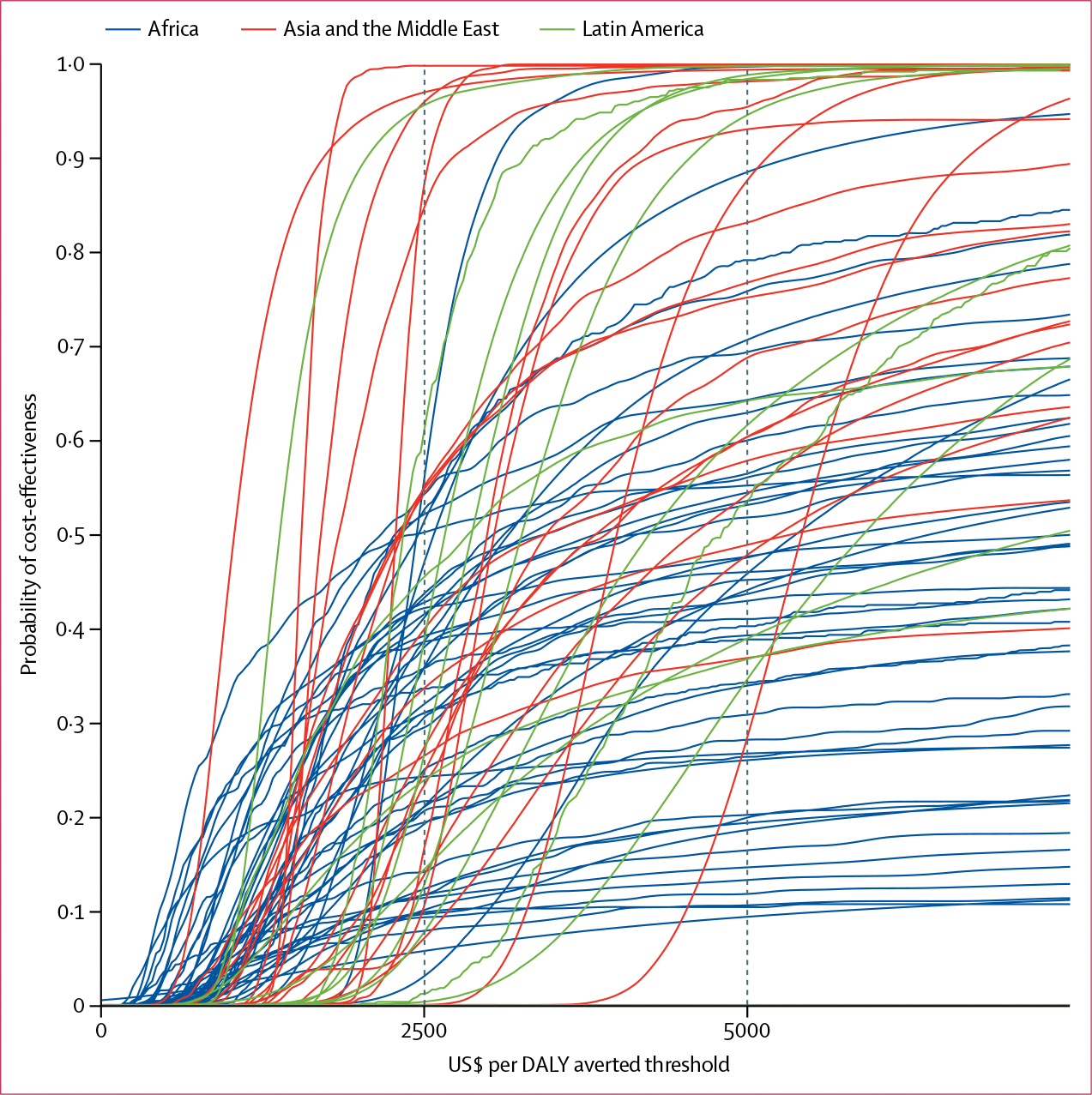
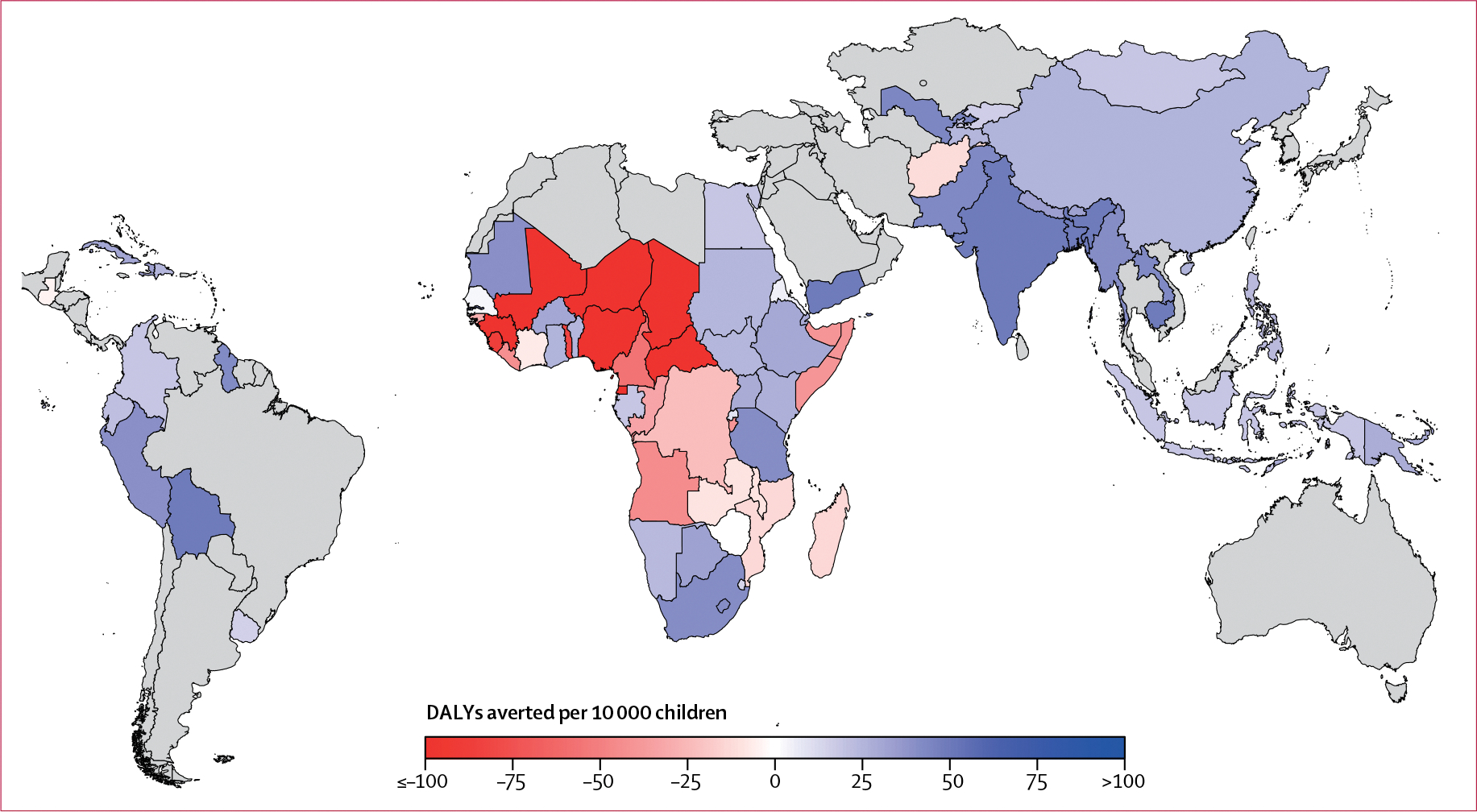
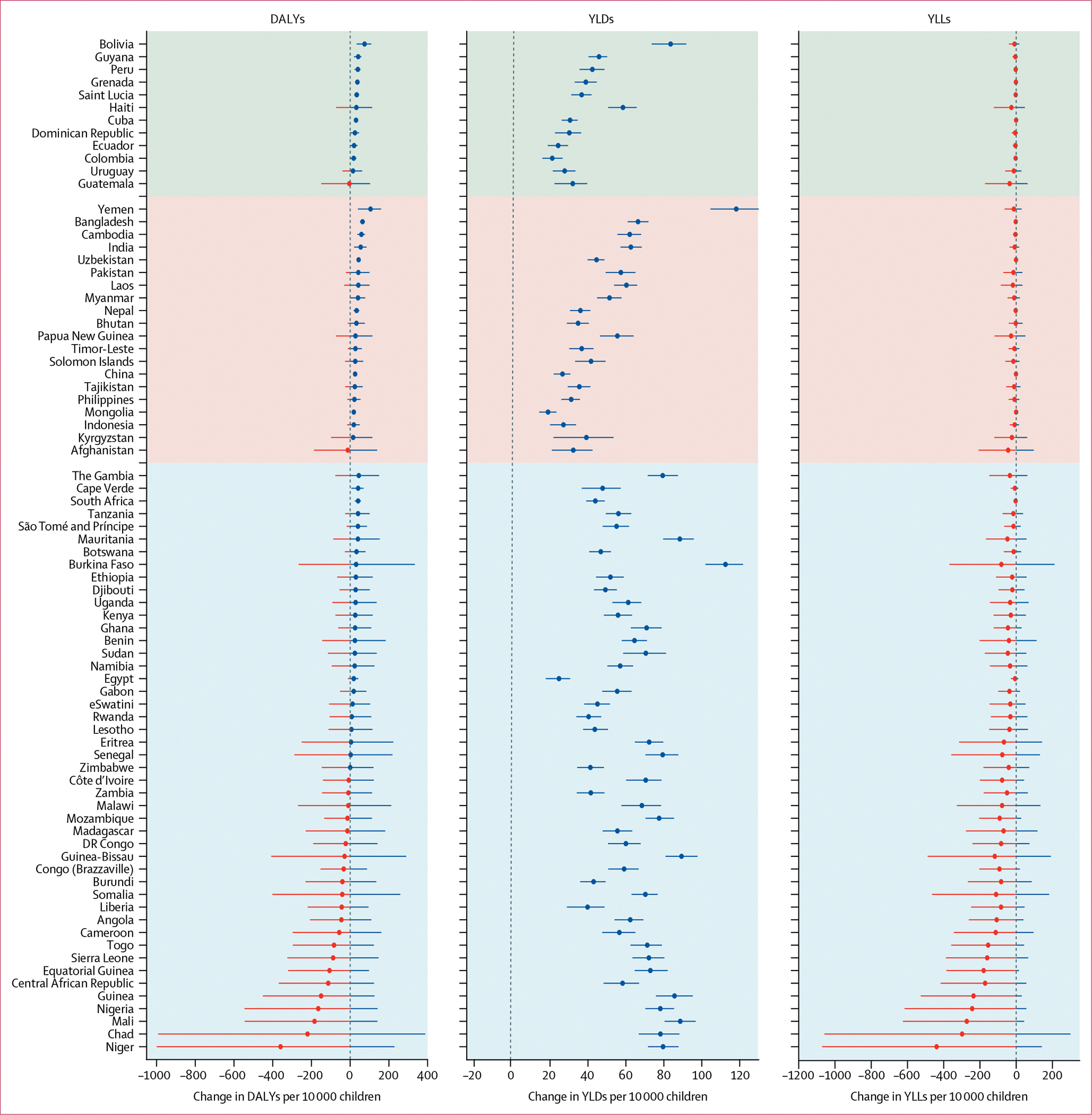
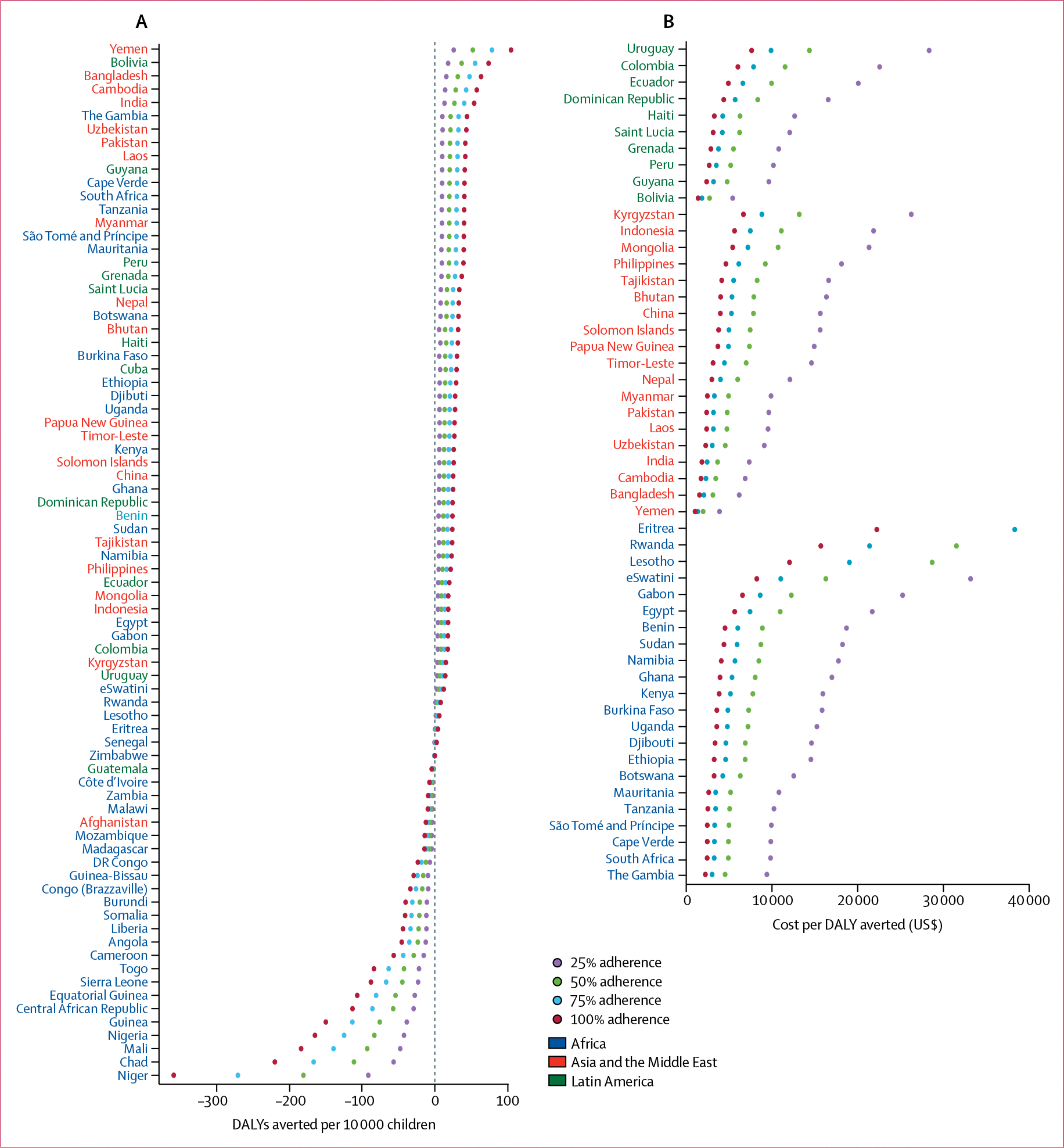
78 countries (46 countries in Africa, 20 in Asia or the Middle East, and 12 in Latin America) were included in the analysis, and we simulated 5 million children per country. 6 months of universal distribution of daily MNPs, assuming 100% coverage, produced a net benefit (DALYs averted) in 54 countries (24 in Africa, 19 in Asia and the Middle East, 11 in Latin America) and net harm in 24 countries (22 in Africa, one in Asia, and one in Latin America). MNP intervention provided a benefit on YLDs associated with anaemia, but these gains were attenuated and sometimes reversed by increases in YLLs associated with malaria and diarrhoea, reducing the benefits seen for DALYs. In the 54 countries where MNP provision was beneficial, the median benefit was 28·1 DALYs averted per 10 000 children receiving MNPs (IQR 20·6-40·4), and median cost per DALY averted was $3576 (IQR 2474-4918). DALY effects positively correlated with moderate and severe anaemia prevalence in Asia, the Middle East, and Latin America, but correlated inversely in Africa. Suboptimal coverage markedly reduced DALYs averted and cost-effectiveness.
Net health benefits of MNPs vary between countries, are highest where prevalence of moderate and severe anaemia is greatest but infection prevalence is smallest, and are ameliorated when coverage of the intervention is poor. Our data provide country-specific guidance to national policy makers.
International Union of Nutrition Sciences.
在中低收入国家,普及用添加铁的多种微量营养素粉(MNP)强化辅食是预防幼儿贫血的关键干预措施。但是,有证据表明 MNP 可能会促进感染,这使得人们对 MNP 是否能带来净健康效益以及是否具有成本效益产生了不确定性。我们旨在确定在中低收入国家,为 6 个月大的儿童普遍提供 MNP 的特定国家的净效益或危害以及成本效益。
我们开发了一个微观模拟模型,以估计因提供为期 6 个月的 MNP 而避免(或增加)的贫血、疟疾和腹泻所导致的特定国家特定的残疾调整生命年(DALY)、残疾生命年(YLD)和生命损失年(YLL),并与不进行干预的情况进行比较,干预组将再随访 6 个月(即至 18 个月)。贫血患病率来自人口与健康调查或类似的全国性调查,疟疾和腹泻的发病率来自全球疾病负担研究。通过建模来确定每避免一个 DALY 的成本(美元)。此外,我们在敏感性分析中探讨了 MNP 覆盖率降低的影响。
78 个国家(46 个非洲国家、20 个亚洲或中东国家和 12 个拉丁美洲国家)被纳入分析,我们模拟了每个国家 500 万儿童。假设 100%的覆盖率,6 个月内普遍分发每日 MNP,在 54 个国家(24 个在非洲、19 个在亚洲和中东、11 个在拉丁美洲)产生了净效益(避免的 DALY),而在 24 个国家(22 个在非洲、1 个在亚洲、1 个在拉丁美洲)产生了净危害。MNP 干预措施对与贫血相关的 YLD 有获益,但这些获益因疟疾和腹泻相关的 YLL 增加而减弱,有时甚至逆转,从而降低了 DALY 的获益。在 MNP 供应有益的 54 个国家中,每 10000 名接受 MNP 的儿童中,MNP 供应的中位数获益为避免 28.1 个 DALY(20.6-40.4),每避免一个 DALY 的成本中位数为 3576 美元(2474-4918)。DALY 效果与亚洲、中东和拉丁美洲的中度和重度贫血患病率呈正相关,但与非洲呈负相关。覆盖范围不理想会大大降低避免的 DALY 数量和成本效益。
MNP 的净健康效益在国家之间存在差异,在中度和重度贫血患病率最高但感染率最低的国家最高,而且在干预措施的覆盖范围较差时,其获益会减轻。我们的数据为国家政策制定者提供了具体的国家指导。
国际营养科学联盟。