From the Department of Epidemiology and Biostatistics (Y.-F.Z., N.L., X.-Y.S., X.-F.P., A.P.), School of Public Health, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China.
Department of Health Economics, School of Public Health, Fudan University, Shanghai, China (P.W.).
Hypertension. 2020 Sep;76(3):750-758. doi: 10.1161/HYPERTENSIONAHA.119.14533. Epub 2020 Jul 27.
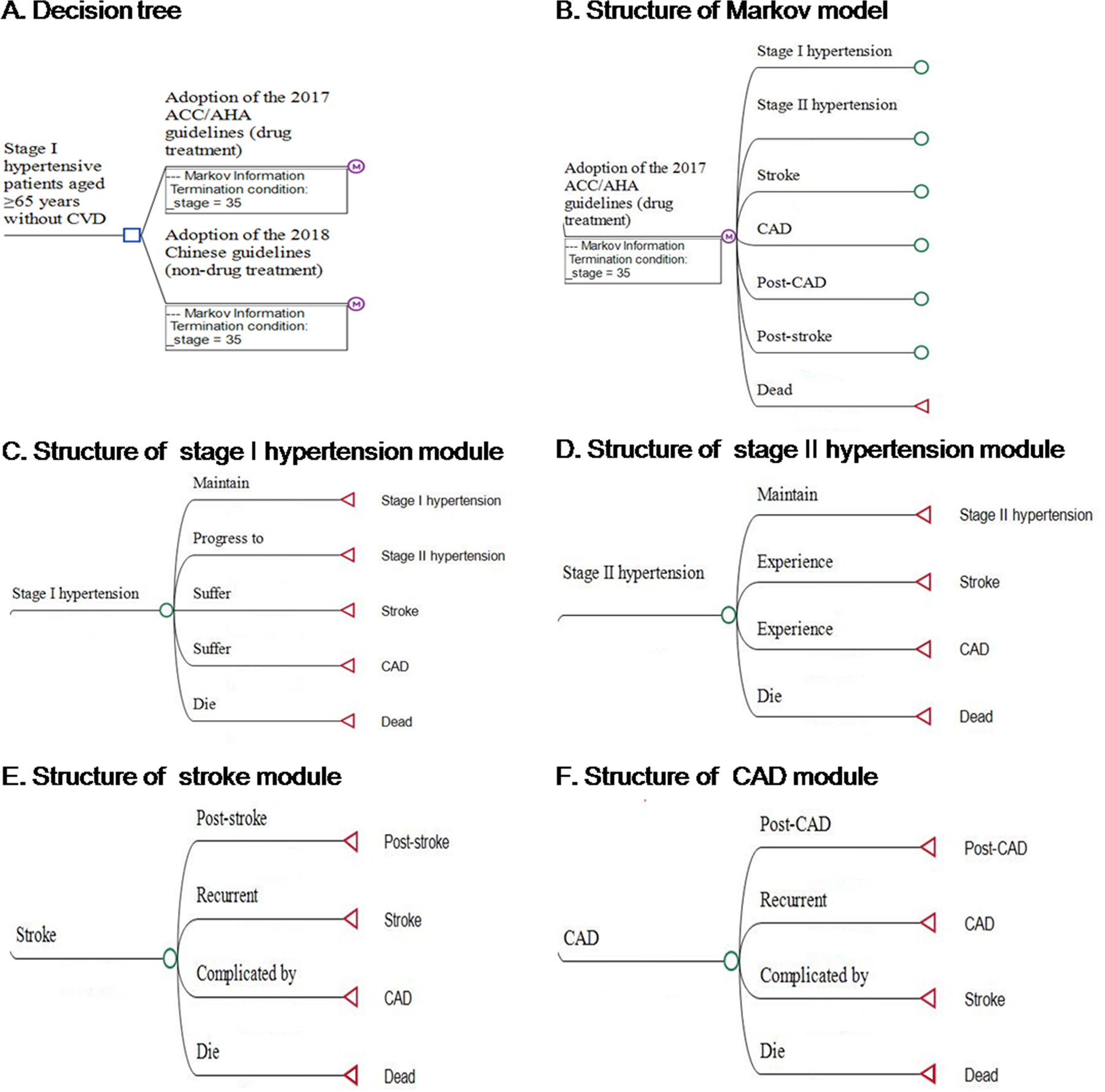
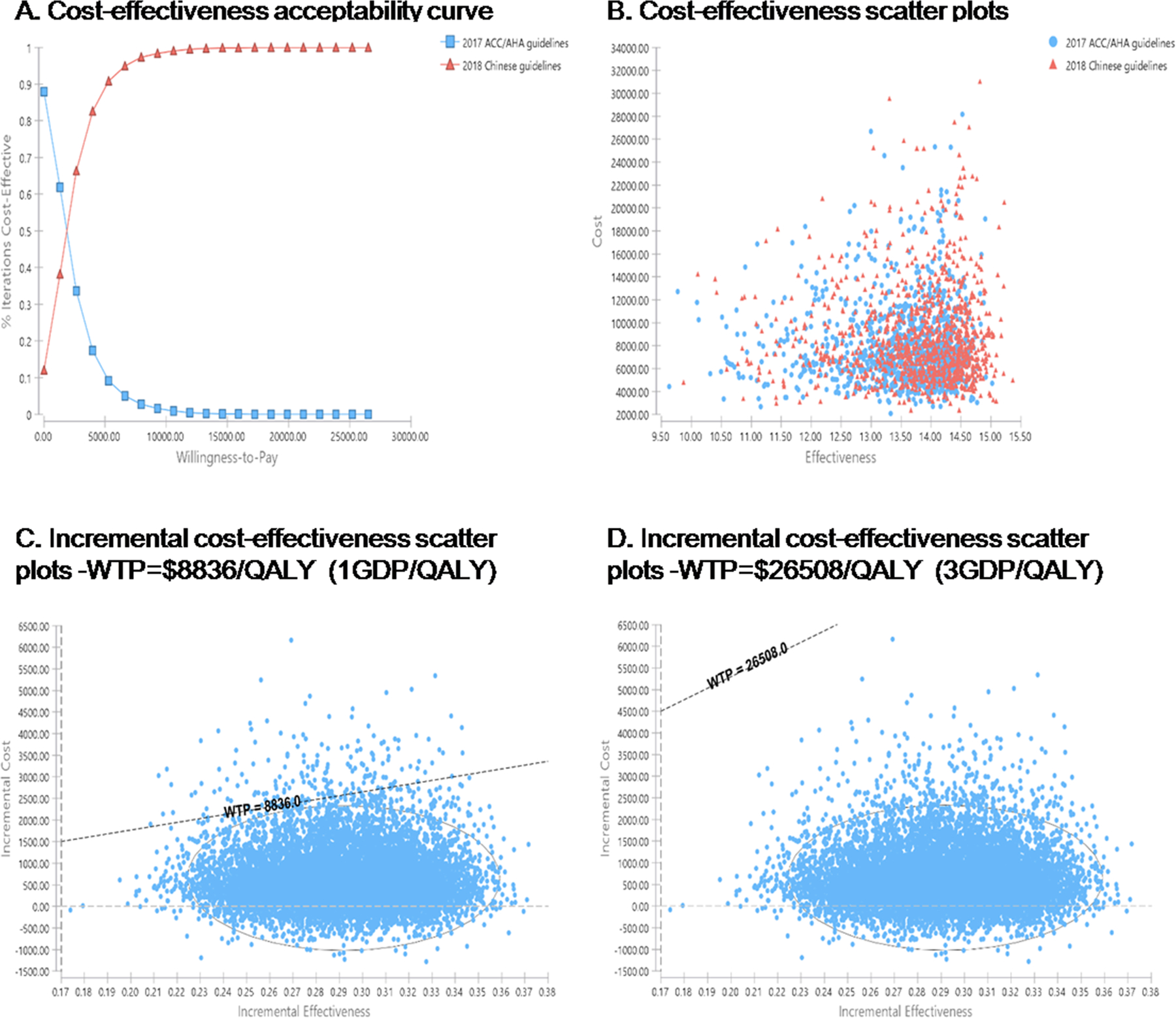
Systolic/diastolic blood pressure of 130 to 139/80 to 89 mm Hg has been defined as stage I hypertension by the 2017 Hypertension Clinical Practice Guidelines. Drug treatment is recommended for stage I hypertensive patients aged ≥65 years without cardiovascular disease in the 2017 Hypertension Clinical Practice Guidelines but not in the 2018 Chinese guidelines. However, the cost-effectiveness of drug treatment among this subgroup of Chinese patients is unclear. This study developed a microsimulation model to compare costs and effectiveness of drug treatment and nondrug treatment for the subgroup of stage I hypertensive patients over a lifetime horizon from a government affordability perspective. Event rates of mortality and cardiovascular complications were estimated from 3 cohorts in the Chinese population. Costs and health utilities were obtained from the national statistics report and published literature. The model predicted that drug treatment generated quality-adjusted life-years of 13.52 and associated with expected costs of $6825 in comparison with 13.81 and $7328 produced by nondrug treatment over a lifetime horizon among stage I hypertensive patients aged ≥65 years without cardiovascular disease. At a willingness-to-pay threshold of $8836/quality-adjusted life-year (the GDP per capita in 2017), drug treatment only had a 1.8% probability of being cost-effective compared with nondrug treatment after 10 000 probabilistic simulations. Sensitivity analysis of treatment costs, benefits expected from treatment, health utilities, and discount rates did not change the results. Our results suggested that drug treatment was not cost-effective compared with nondrug treatment for stage I hypertensive patients aged ≥65 years without cardiovascular disease in China.
收缩压/舒张压为 130 至 139/80 至 89mmHg 已被 2017 年高血压临床实践指南定义为 1 期高血压。2017 年高血压临床实践指南建议对年龄≥65 岁且无心血管疾病的 1 期高血压患者进行药物治疗,但 2018 年中国指南则不建议这样做。然而,对于中国患者的这一亚组人群,药物治疗的成本效益尚不清楚。本研究从政府支付能力的角度出发,开发了一个微观模拟模型,比较了药物治疗和非药物治疗在终生范围内对无心血管疾病的≥65 岁 1 期高血压患者亚组的成本效益。死亡率和心血管并发症的事件发生率是根据中国人群中的 3 个队列估计的。成本和健康效用是从国家统计报告和已发表的文献中获得的。模型预测,与非药物治疗相比,药物治疗在 1 期高血压患者中(无心血管疾病)≥65 岁的患者亚组中,在终生范围内产生的质量调整生命年为 13.52 年,预计成本为 6825 美元,而产生的质量调整生命年为 13.81 年,预计成本为 7328 美元。在 8836 美元/质量调整生命年(2017 年人均 GDP)的意愿支付阈值下,在 10000 次概率模拟后,药物治疗仅比非药物治疗具有 1.8%的成本效益可能性。治疗成本、治疗预期收益、健康效用和贴现率的敏感性分析并未改变结果。研究结果表明,在中国,与非药物治疗相比,药物治疗对无心血管疾病的≥65 岁 1 期高血压患者并不具有成本效益。