Pinheiro Fillipe Dantas, Teixeira Adriano Fernandes, de Brito Breno Bittencourt, da Silva Filipe Antônio França, Santos Maria Luísa Cordeiro, de Melo Fabrício Freire
Instituto Multidisciplinar em Saúde, Universidade Federal da Bahia, Vitória da Conquista 45029-094, Bahia, Brazil.
World J Clin Oncol. 2020 May 24;11(5):250-259. doi: 10.5306/wjco.v11.i5.250.
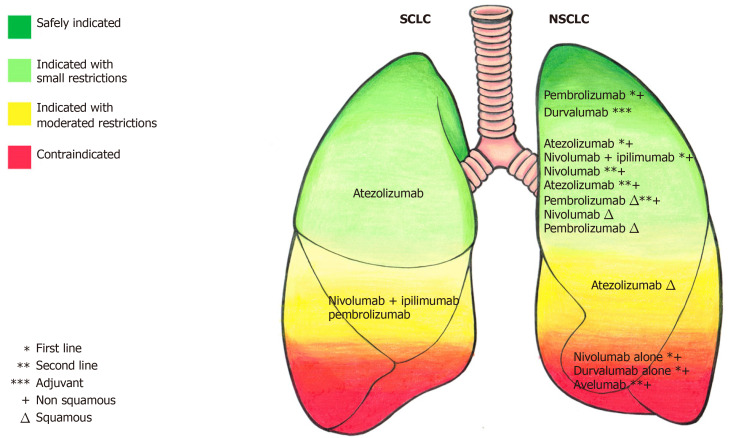
Lung carcinoma is associated with a high mortality worldwide, being the leading cause of cancer death. It is mainly classified into squamous non-small cell lung cancer (NSCLC), non-squamous NSCLC, and small cell lung cancer. However, such malignancy has been increasingly subdivided into histological and molecular subtypes to guide treatment. Therapies can be used in adjuvant and palliative settings. Regarding immunotherapy, it has been widely tested in both first or subsequent palliative lines. In this sense, drugs such as pembrolizumab, nivolumab, atezolizumab, ipilimumab, avelumab, and durvalumab have been assessed in large studies. Some of these trials have also studied these medicines in adjuvant and in maintenance therapy. In recent years, advances in immunotherapy have raised the hope that the unfavorable prognosis observed in several affected individuals can be changed. Immunotherapy has increased the overall survival in squamous NSCLC, non-squamous NSCLC, and small cell lung cancer. However, it has added to the oncology practice some side effects that are unusual in standard chemotherapy and require special clinical support. In order to show how immunotherapy is being applied in the treatment of lung carcinoma, we reviewed the main studies in adjuvant and palliative scenarios. What is the better scheme? What is the better combination? What is the better dose? When should we use immunotherapy? Does programmed cell death ligand 1 expression significantly interfere in immunotherapy efficiency? Some of these questions have already been answered, while others require more investigations.
肺癌在全球范围内与高死亡率相关,是癌症死亡的主要原因。它主要分为鳞状非小细胞肺癌(NSCLC)、非鳞状NSCLC和小细胞肺癌。然而,这种恶性肿瘤已越来越多地细分为组织学和分子亚型以指导治疗。治疗可用于辅助和姑息治疗。关于免疫疗法,它已在一线或后续姑息治疗中得到广泛测试。从这个意义上说,派姆单抗、纳武单抗、阿特珠单抗、伊匹单抗、阿维鲁单抗和度伐鲁单抗等药物已在大型研究中得到评估。其中一些试验还研究了这些药物在辅助治疗和维持治疗中的效果。近年来,免疫疗法的进展带来了希望,即一些受影响个体中观察到的不良预后可以得到改变。免疫疗法提高了鳞状NSCLC、非鳞状NSCLC和小细胞肺癌的总生存率。然而,它给肿瘤学实践带来了一些在标准化疗中不常见的副作用,需要特殊的临床支持。为了展示免疫疗法在肺癌治疗中的应用方式,我们回顾了辅助和姑息治疗场景中的主要研究。哪种方案更好?哪种组合更好?哪种剂量更好?我们应该何时使用免疫疗法?程序性细胞死亡配体1的表达是否会显著影响免疫疗法的疗效?其中一些问题已经得到解答,而其他问题则需要更多研究。