Department of Radiology, Division of Pediatric Radiology, Montefiore Medical Center, 111 E. 210th St., Bronx, NY, 10467, USA.
Pediatr Radiol. 2020 Sep;50(10):1369-1374. doi: 10.1007/s00247-020-04782-2. Epub 2020 Jul 29.
Coronavirus disease 2019 (COVID-19) primarily affects adults, with a lower incidence in children.
To report our experience with critically ill children with COVID-19.
We reviewed the medical records of children with COVID-19 who were admitted Feb. 25 to May 1, 2020. We reviewed patient demographics, symptoms, comorbidities, requirement for respiratory support, evidence of acute myocardial injury, and chest radiographs.
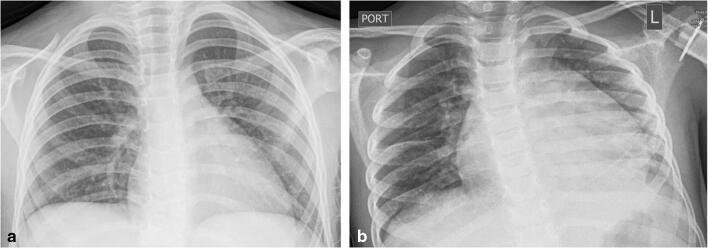
The study included 19 children and adolescents (ages 2 months to 18 years, median 8 years; 10 males, 9 females; 18 COVID-19-positive, 1 COVID-19-negative with positive exposure). Presenting symptoms included fever (89%), cough (68%), respiratory distress (68%) and vomiting/diarrhea (47%). Comorbidities were present in 12 (63%). Fourteen required intensive care; eight required intubation. Two children died. Five patients developed acute myocarditis (median age 7 years); in all five, chest radiographs were notable for cardiomegaly and pulmonary congestion or interstitial edema. Of these five, one (age 18 years), who had underlying hypertension and obesity, developed multifocal pneumonia and renal failure. The other four were previously healthy; three (ages 5 years, 7 years, 8 years) were subsequently diagnosed with multisystemic inflammatory syndrome in children (MIS-C); one developed pulmonary opacities consistent with adult respiratory distress syndrome, three (60%) had no parenchymal pulmonary opacities. Fourteen patients (median 13 years), most with comorbidities, had no acute myocardial injury. Chest radiographs in 13 (93%) demonstrated parenchymal lung disease with a predominant perihilar and basilar distribution.
Myocarditis without pulmonary disease occurred in children in their first decade as a component of MIS-C, a newly described syndrome of multisystemic inflammation requiring further investigation. Pulmonary disease dominated the radiographic features of COVID-19-positive adolescents in their second decade in whom radiographs demonstrated predominantly perihilar and basilar distribution of lung opacities.
2019 年冠状病毒病(COVID-19)主要影响成年人,儿童发病率较低。
报告我们在 COVID-19 危重症儿童方面的经验。
我们回顾了 2020 年 2 月 25 日至 5 月 1 日期间收治的 COVID-19 患儿的病历。我们回顾了患者的人口统计学资料、症状、合并症、呼吸支持需求、急性心肌损伤证据和胸部 X 线片。
本研究纳入 19 例 2 个月至 18 岁(中位年龄 8 岁;男 10 例,女 9 例;COVID-19 阳性 18 例,COVID-19 阴性但有阳性接触者 1 例)患儿和青少年。首发症状包括发热(89%)、咳嗽(68%)、呼吸窘迫(68%)和呕吐/腹泻(47%)。合并症见于 12 例(63%)。14 例需要重症监护;8 例需要插管。2 例患儿死亡。5 例患儿发生急性心肌炎(中位年龄 7 岁);所有 5 例患儿的胸部 X 线片均有心脏增大和肺淤血或间质性水肿。其中 1 例(18 岁),患有高血压和肥胖症,并发多灶性肺炎和肾衰竭。其余 4 例患儿均为既往健康;其中 3 例(5 岁、7 岁、8 岁)诊断为儿童多系统炎症综合征(MIS-C);1 例患儿出现符合成人呼吸窘迫综合征的肺部混浊,3 例(60%)患儿肺部实质混浊。14 例(中位年龄 13 岁)患儿,大多数合并症,无急性心肌损伤。13 例(93%)患儿的胸部 X 线片显示肺实质疾病,主要分布在肺门周围和基底部分。
在作为 MIS-C 组成部分的儿童的第一个十年中,无肺部疾病的心肌炎是一种新描述的多系统炎症综合征,需要进一步研究。在第二个十年的 COVID-19 阳性青少年中,肺部疾病是放射学特征的主要表现,胸部 X 线片显示肺门周围和基底部分为主的肺不张。