Blood and Marrow Transplantation, H. Lee Moffitt Cancer Center and Research Institute, Tampa, FL, USA.
Department of Oncology, University of Alberta, Edmonton, Alberta, Canada.
J Cachexia Sarcopenia Muscle. 2020 Dec;11(6):1570-1579. doi: 10.1002/jcsm.12604. Epub 2020 Jul 29.
Quantification of skeletal muscle using computed tomography (CT) is accessible using cancer patients' standard oncologic images. Reduced muscle mass may be related to reduced respiratory muscle strength; however, the impact of this on lung functional parameters is not characterized in adult allogeneic haematopoietic stem cell transplant (alloHCT) recipients.
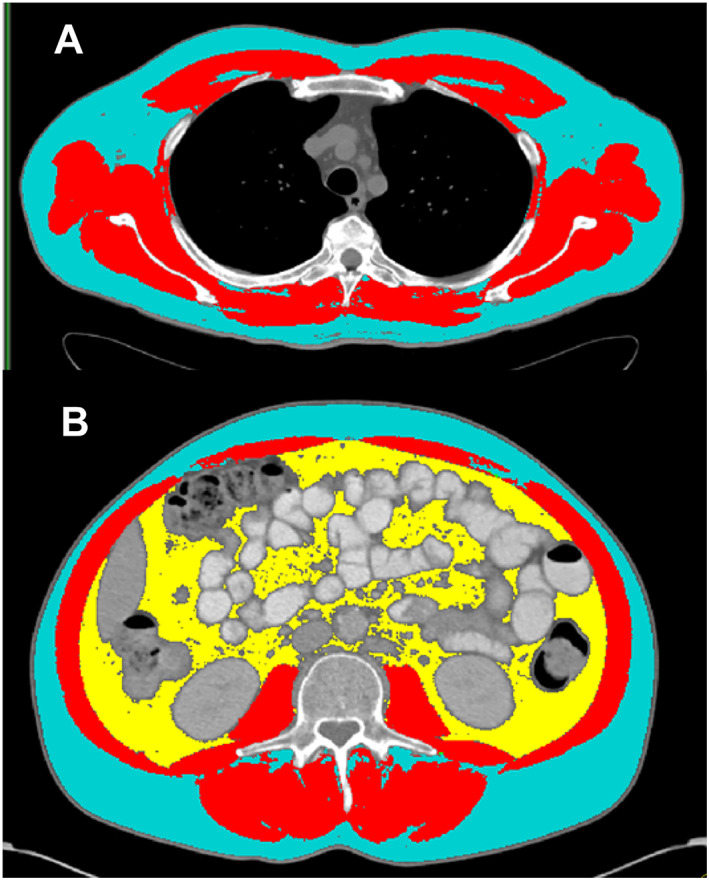
A consecutive retrospective series (n = 296) of patients who had alloHCT at a comprehensive cancer centre between March 2005 and April 2015 were included. Pre-transplant CT scans were used to quantify skeletal muscle and adipose tissue at the fourth thoracic (T4) and/or third lumbar (L3) level. Tumour and patient characteristics were recorded, including forced expiratory volume in 1 second (FEV ) by spirometry. Regression models were created to characterize predictive relationships.
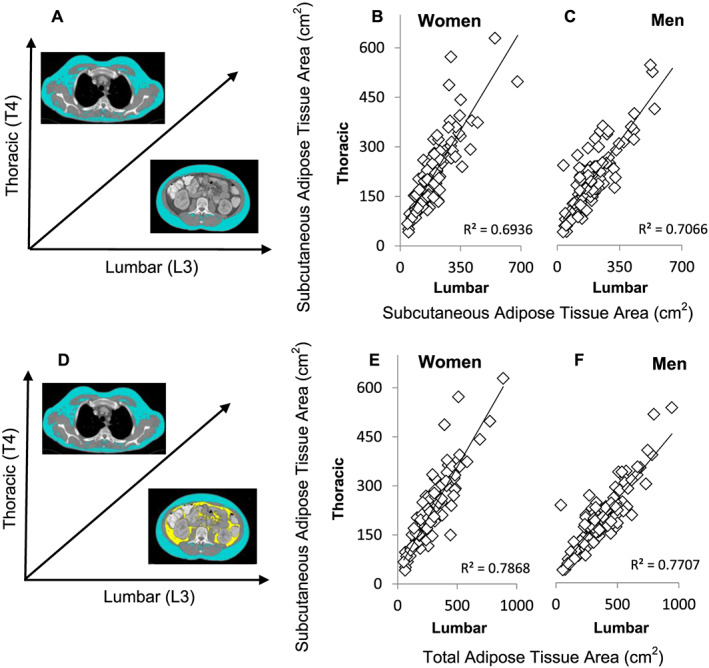
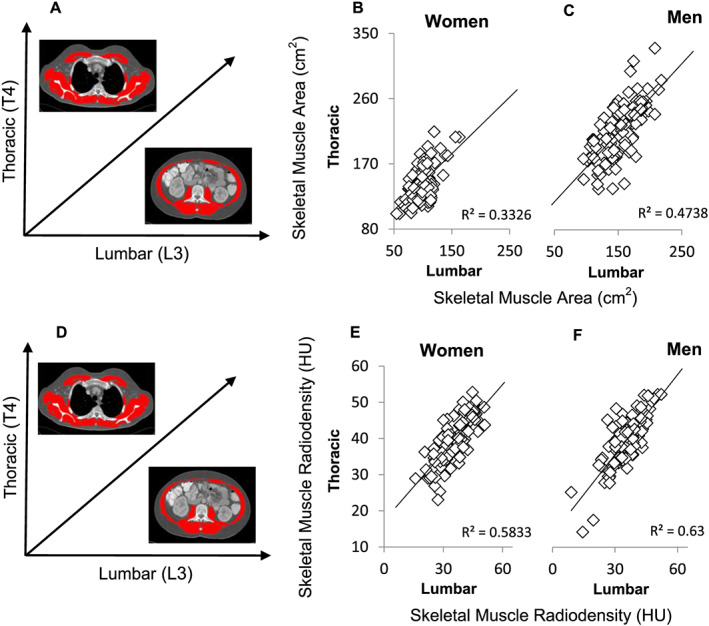
A total of 296 patients (♂n = 161; ♀n = 135) were included, all of whom had chest CT as part of standard care; a subset of these (n = 215, 72.6%) also had abdominal CT. Diagnoses were non-Hodgkins lymphoma (n = 165), acute myeloid leukaemia (n = 66), Hodgkin's disease (n = 14), acute lymphocytic leukaemia (n = 14), myelodysplastic syndromes (n = 18), and other (n = 19). In multivariable linear regression adjusted for sex (P < 0.0001), age (P < 0.0001), haematopoietic cell transplantation-specific co-morbidity index (P = 0.010), and parameters of pulmonary function testing (defined by spirometry, P < 0.0001), both T4 muscle index [β 0.127 (95% confidence interval 0.019; 0.252), P < 0.0001] and T4 muscle radiodensity [β 0.132 (95% confidence interval 0.087; 0.505), P = 0.006] were independently associated with FEV ; disease risk index (P = 0.877) and Karnofsky performance status (P = 0.548) were not associated with FEV . Similar conclusions were obtained when L3 muscle index and radiodensity were considered. Unlike T4, L3 muscle index values can be compared with published cut-off values for sarcopenia. Overall rates of sarcopenia were uniformly higher in the HCT population than in age-matched and sex-matched patients with solid tumours [alloHCT ♂64.7% vs. solid tumour ♂56.6% (P < 0.001); alloHCT ♀57.6% vs. solid tumour ♀36.0% (P < 0.001)]. Significant but moderate correlations (P < 0.001) were found for muscle area and radiodensity between L3 and T4, for both men and women; adipose tissue quantity also correlated significantly (P < 0.001) between L3 and T4 for both men and women.
Lumbar or thoracic CT images are useful for body composition assessment in this population and reveal high rates of sarcopenia, similar to those reported in very elderly patients. Reduced muscle mass and radiodensity associate with impaired FEV even after adjustment for clinical covariables including co-morbidities, performance status, disease risk, and mild intrinsic pulmonary disease (chronic obstructive pulmonary disease) defined by spirometry.
使用计算机断层扫描(CT)对骨骼肌肉进行量化在癌症患者的标准肿瘤图像中是可行的。肌肉减少可能与呼吸肌强度降低有关;然而,在接受异体造血干细胞移植(alloHCT)的成年患者中,其对肺功能参数的影响尚未确定。
本研究纳入了 2005 年 3 月至 2015 年 4 月在一家综合性癌症中心接受 alloHCT 的连续回顾性系列(n=296)患者。在移植前使用 CT 扫描来量化第 4 胸椎(T4)和/或第 3 腰椎(L3)水平的骨骼肌和脂肪组织。记录了肿瘤和患者特征,包括通过肺活量计测量的第 1 秒用力呼气量(FEV )。建立了回归模型来描述预测关系。
共纳入 296 例患者(♂n=161;♀n=135),所有患者均接受了胸部 CT 作为标准治疗的一部分;其中一部分(n=215,72.6%)还接受了腹部 CT。诊断包括非霍奇金淋巴瘤(n=165)、急性髓系白血病(n=66)、霍奇金病(n=14)、急性淋巴细胞白血病(n=14)、骨髓增生异常综合征(n=18)和其他(n=19)。在多变量线性回归中,校正性别(P<0.0001)、年龄(P<0.0001)、造血细胞移植特异性合并症指数(P=0.010)和肺功能测试参数(通过肺活量计定义,P<0.0001)后,T4 肌肉指数[β 0.127(95%置信区间 0.019;0.252),P<0.0001]和 T4 肌肉密度[β 0.132(95%置信区间 0.087;0.505),P=0.006]与 FEV 独立相关;疾病风险指数(P=0.877)和卡诺夫斯基表现状态(P=0.548)与 FEV 无关。当考虑 L3 肌肉指数和密度时,得出了类似的结论。与 T4 不同,L3 肌肉指数值可以与发表的肌肉减少症截断值进行比较。与年龄和性别匹配的实体瘤患者相比,HCT 人群的肌肉减少症总体发生率更高[alloHCT♂64.7%比实体瘤♂56.6%(P<0.001);alloHCT♀57.6%比实体瘤♀36.0%(P<0.001)]。在男性和女性中,均发现 L3 和 T4 之间的肌肉面积和密度存在显著但中度相关(P<0.001);男女之间的脂肪组织量也存在显著相关(P<0.001)。
腰椎或胸椎 CT 图像可用于该人群的身体成分评估,并显示出与非常老年患者相似的高肌肉减少症发生率。即使在调整了包括合并症、表现状态、疾病风险和通过肺活量计定义的轻度固有肺疾病(慢性阻塞性肺疾病)在内的临床协变量后,肌肉减少和密度降低仍与 FEV 受损相关。