US Centers for Disease Control and Prevention, Atlanta, Georgia, USA.
Department of Epidemiology and Biostatistics, CUNY Graduate School of Public Health & Health Policy, New York, USA.
Clin Infect Dis. 2021 Oct 5;73(7):e2217-e2225. doi: 10.1093/cid/ciaa1068.
Children living with human immunodeficiency virus (HIV) (CLHIV) receiving antiretroviral therapy (ART) in resource-limited settings are susceptible to high rates of acquired HIV drug resistance (HIVDR), but few studies include children initiating age-appropriate World Health Organization (WHO)-recommended first-line regimens. We report data from a cohort of ART-naive South African children who initiated first-line ART.
ART-eligible CLHIV aged 0-12 years were enrolled from 2012 to 2014 at 5 public South African facilities and were followed for up to 24 months. Enrolled CLHIV received standard-of-care WHO-recommended first-line ART. At the final study visit, a dried blood spot sample was obtained for viral load and genotypic resistance testing.
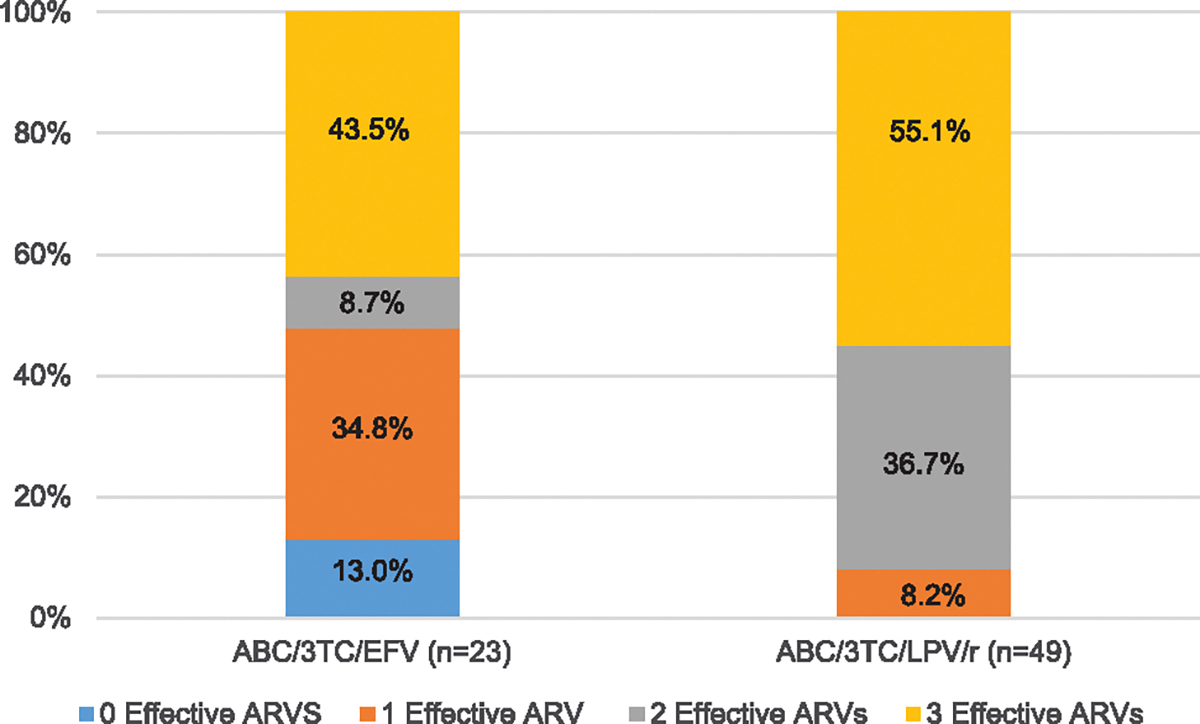
Among 72 successfully genotyped CLHIV, 49 (68.1%) received ABC/3TC/LPV/r, and 23 (31.9%) received ABC/3TC/EFV. All but 2 children on ABC/3TC/LPV/r were <3 years, and all CLHIV on ABC/3TC/EFV were ≥3 years. Overall, 80.6% (58/72) had at least one drug resistance mutation (DRM). DRMs to nonnucleoside reverse transcriptase inhibitors (NNRTIs) and nucleoside reverse transcriptase inhibitors (NRTIs) were found among 65% and 51% of all CLHIV, respectively, with no statistical difference by ART regimen. More CLHIV on ABC/3TC/EFV, 47.8% (11/23), were found to have 0 or only 1 effective antiretroviral drug remaining in their current regimen compared to 8.2% (4/49) on ABC/3TC/LPV/r.
High levels of NNRTI and NRTI DRMs among CLHIV receiving ABC/3TC/LPV/r suggests a lasting impact of failed mother-to-child transmission interventions on DRMs. However, drug susceptibility analysis reveals that CLHIV with detectable viremia on ABC/3TC/LPV/r are more likely to have maintained at least 2 effective agents on their current HIV regimen than those on ABC/3TC/EFV.
在资源有限的环境中,接受抗逆转录病毒疗法(ART)的携带人类免疫缺陷病毒(HIV)的儿童(CLHIV)易发生获得性 HIV 耐药性(HIVDR),但很少有研究包括开始接受世卫组织推荐的适合年龄的一线方案的儿童。我们报告了一项在南非接受 ART 治疗的天真儿童队列中的数据。
2012 年至 2014 年,从南非 5 家公立医疗机构招募了年龄在 0-12 岁的符合 ART 条件的 CLHIV,并对其进行了长达 24 个月的随访。入组的 CLHIV 接受了标准的世卫组织推荐的一线 ART。在最后一次研究访问时,采集了干血斑样本进行病毒载量和基因型耐药性检测。
在 72 名成功进行基因分型的 CLHIV 中,49 名(68.1%)接受 ABC/3TC/LPV/r,23 名(31.9%)接受 ABC/3TC/EFV。除了 2 名接受 ABC/3TC/LPV/r 的儿童外,所有儿童均<3 岁,而所有接受 ABC/3TC/EFV 的儿童均≥3 岁。总体而言,80.6%(58/72)存在至少一种耐药突变(DRM)。所有 CLHIV 中分别有 65%和 51%存在非核苷类逆转录酶抑制剂(NNRTIs)和核苷类逆转录酶抑制剂(NRTIs)耐药,两种方案之间无统计学差异。在接受 ABC/3TC/EFV 的儿童中,47.8%(11/23)发现其当前方案中仅剩 0 种或仅 1 种有效的抗逆转录病毒药物,而接受 ABC/3TC/LPV/r 的儿童中仅有 8.2%(4/49)。
在接受 ABC/3TC/LPV/r 的 CLHIV 中,NNRTI 和 NRTI 耐药率较高,表明母婴传播干预失败对耐药性的持续影响。然而,药物敏感性分析显示,在 ABC/3TC/LPV/r 上检测到病毒血症的 CLHIV 比接受 ABC/3TC/EFV 的 CLHIV 更有可能在其当前的 HIV 方案中保留至少 2 种有效的药物。