Department of Intensive Care Unit, The First Hospital of Jilin University, Changchun, 130021, Jilin, China.
Crit Care. 2020 Aug 6;24(1):488. doi: 10.1186/s13054-020-03204-x.
The effect of the timing of norepinephrine initiation on clinical outcomes in patients with septic shock is uncertain. A systematic review and meta-analysis was performed to evaluate the impact of early and late start of norepinephrine support on clinical outcomes in patients with septic shock.
We searched the PubMed, Cochrane, and Embase databases for randomized controlled trials (RCTs) and cohort studies from inception to the 1st of March 2020. We included studies involving adult patients (> 18 years) with septic shock. All authors reported our primary outcome of short-term mortality and clearly comparing early versus late norepinephrine initiation with clinically relevant secondary outcomes (ICU length of stay, time to achieved target mean arterial pressure (≥ 65 mmHg), and volume of intravenous fluids within 6 h). Results were expressed as odds ratio (OR) and mean difference (MD) with accompanying 95% confidence interval (CI).
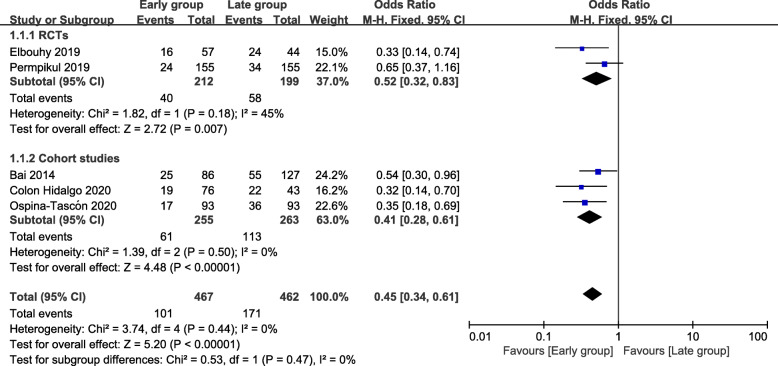
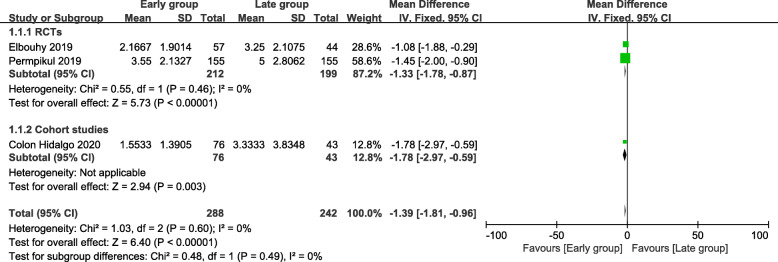
Five studies including 929 patients were included. The primary outcome of this meta-analysis showed that the short-term mortality of the early group was lower than that of the late group (odds ratio [OR] = 0.45; 95% CI, 0.34 to 0.61; P < 0.00001; χ = 3.74; I = 0%). Secondary outcomes demonstrated that the time to achieved target MAP of the early group was shorter than that of the late group (mean difference = - 1.39; 95% CI, - 1.81 to - 0.96; P < 0.00001; χ = 1.03; I = 0%). The volume of intravenous fluids within 6 h of the early group was less than that of the late group (mean difference = - 0.50; 95% CI, - 0.68 to - 0.32; P < 0.00001; χ = 33.76; I = 94%). There was no statistically significant difference in the ICU length of stay between the two groups (mean difference = - 0.11; 95% CI, - 1.27 to 1.05; P = 0.86; χ = 0.85; I = 0%).
Early initiation of norepinephrine in patients with septic shock was associated with decreased short-term mortality, shorter time to achieved target MAP, and less volume of intravenous fluids within 6 h. There was no significant difference in ICU length of stay between early and late groups. Further large-scale RCTs are still required to confirm these results.
去甲肾上腺素起始时机对脓毒性休克患者临床结局的影响尚不确定。本系统评价和荟萃分析旨在评估脓毒性休克患者早期和晚期开始使用去甲肾上腺素支持对临床结局的影响。
我们检索了从建库到 2020 年 3 月 1 日的 PubMed、Cochrane 和 Embase 数据库中的随机对照试验(RCT)和队列研究。我们纳入了涉及脓毒性休克成年患者(>18 岁)的研究。所有作者报告了我们的主要结局即短期死亡率,并明确比较了早期与晚期开始使用去甲肾上腺素与具有临床意义的次要结局(ICU 住院时间、达到目标平均动脉压(≥65mmHg)的时间和 6 小时内静脉输液量)。结果以比值比(OR)和均数差(MD)及其伴随的 95%置信区间(CI)表示。
共纳入了 5 项研究,共计 929 例患者。荟萃分析的主要结局显示,早期组的短期死亡率低于晚期组(OR=0.45;95%CI,0.34 至 0.61;P<0.00001;χ²=3.74;I²=0%)。次要结局表明,早期组达到目标 MAP 的时间短于晚期组(MD=-1.39;95%CI,-1.81 至 -0.96;P<0.00001;χ²=1.03;I²=0%)。早期组在 6 小时内的静脉输液量少于晚期组(MD=-0.50;95%CI,-0.68 至 -0.32;P<0.00001;χ²=33.76;I²=94%)。两组 ICU 住院时间无统计学差异(MD=-0.11;95%CI,-1.27 至 1.05;P=0.86;χ²=0.85;I²=0%)。
在脓毒性休克患者中早期开始使用去甲肾上腺素可降低短期死亡率、达到目标 MAP 的时间缩短、6 小时内静脉输液量减少。早期组和晚期组 ICU 住院时间无显著差异。仍需要进一步的大规模 RCT 来证实这些结果。