Alexander Suceena, Yusuf Sabina, Rajan Gautham, Elias John Elenjickal, Roy Sanjeet, Annamalai V C, Thomas Athul, Joseph Eapen Jeethu, T Valson Anna, George David Vinoi, Varughese Santosh
Department of Nephrology, Christian Medical College, Vellore, Tamil Nadu, 632004, India.
Department of General Pathology, Christian Medical College, Vellore, Tamil Nadu, 632004, India.
Wellcome Open Res. 2020 Jul 8;5:164. doi: 10.12688/wellcomeopenres.16071.1. eCollection 2020.
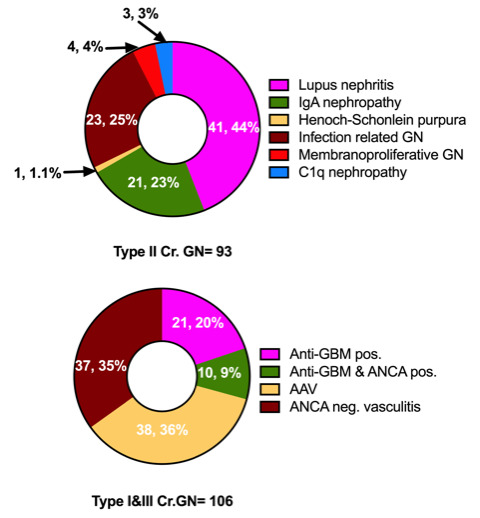
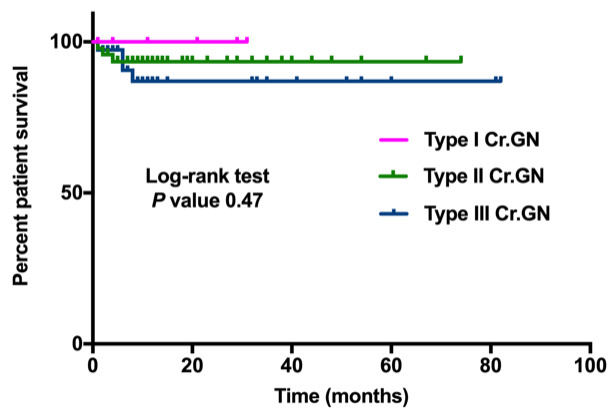
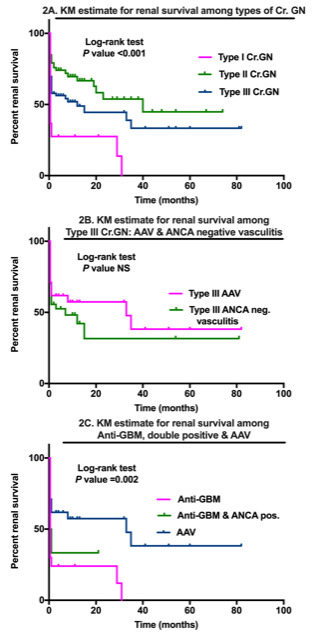
The spectrum and outcomes of crescentic glomerulonephritis (Cr.GN) in South Asia is vastly different from that reported worldwide and there is a paucity of information. The aim of the study was to study the demography, clinical presentation, histology and predictors of longitudinal outcomes of Cr.GN in this population. An observational cohort study of renal biopsies was performed in the largest tertiary center in South India over a period of 10 years (January 2006 to December 2015) with ≥50% crescents on renal histology indicating Cr.GN. A total of 8645 kidney biopsies were done; 200 (2.31%) were Cr.GN. Patients were categorized into three etiological groups: anti-glomerular basement membrane (type I), immune complex (type II), and pauci-immune (type III). Type II was the most common (96, 46.5%), followed by type III (73, 38%) and type I (31, 15.5%). Female preponderance was seen across all types. About half of all patients presented with recent onset hypertension. Type II had the highest median proteinuria (4.2 (2.1-6) g/day, p=0.06) and the median estimated glomerular filtration rate was lowest in type I (5 (4-8) ml/min/1.73m , p<0.001). Among type III, anti-neutrophil cytoplasmic antibodies (ANCA)-associated vasculitis was seen only in ~50% of patients. Nearly one third of patients with type I were also positive for ANCA making them 'double positive'. Acute glomerular insults like tuft necrosis and chronic changes as evidenced by moderate to severe interstitial fibrosis, was a predominant feature of type I. ANCA-negative pauci-immune vasculitis, as well as double positive Cr.GN, are reported for the first time in South-Asia. Renal survival was significantly worse in type I/III compared to type II. Types I/III, moderate to severe interstitial fibrosis and tubular atrophy, presence of oliguria/anuria and increasing percentage of crescents in renal biopsy were significant predictors of end stage kidney disease in our cohort.
南亚新月体性肾小球肾炎(Cr.GN)的谱系和结局与全球报道的情况有很大不同,且相关信息匮乏。本研究的目的是研究该人群中Cr.GN的人口统计学、临床表现、组织学及纵向结局的预测因素。在印度南部最大的三级中心进行了一项为期10年(2006年1月至2015年12月)的肾脏活检观察性队列研究,肾脏组织学检查显示≥50%的新月体则表明为Cr.GN。共进行了8645例肾脏活检;其中200例(2.31%)为Cr.GN。患者被分为三个病因组:抗肾小球基底膜(I型)、免疫复合物(II型)和寡免疫(III型)。II型最为常见(96例,46.5%),其次是III型(73例,38%)和I型(31例,15.5%)。所有类型均以女性居多。约一半的患者近期出现高血压。II型蛋白尿中位数最高(4.2(2.1 - 6)g/天,p = 0.06),I型的估计肾小球滤过率中位数最低(5(4 - 8)ml/min/1.73m²,p < 0.001)。在III型中,仅约50%的患者可见抗中性粒细胞胞浆抗体(ANCA)相关性血管炎。I型患者中近三分之一的ANCA也呈阳性,使其成为“双阳性”。急性肾小球损伤如肾小球毛细血管襻坏死以及中度至重度间质纤维化所证实的慢性改变,是I型的主要特征。南亚首次报道了ANCA阴性的寡免疫性血管炎以及双阳性Cr.GN。与II型相比,I/III型的肾脏生存率明显更差。在我们的队列中,I/III型、中度至重度间质纤维化和肾小管萎缩、少尿/无尿的存在以及肾脏活检中新月体百分比增加是终末期肾病的重要预测因素。