Hinman Rana S, Kimp Alexander J, Campbell Penny K, Russell Trevor, Foster Nadine E, Kasza Jessica, Harris Anthony, Bennell Kim L
Centre for Health, Exercise and Sports Medicine, Department of Physiotherapy, School of Health Sciences, Faculty of Medicine Dentistry & Health Sciences, The University of Melbourne, Melbourne, Australia.
RECOVER Injury Research Centre, The University of Queensland, Brisbane, Australia.
BMC Musculoskelet Disord. 2020 Aug 7;21(1):522. doi: 10.1186/s12891-020-03523-8.
Knee osteoarthritis (OA) is a global problem that causes significant pain and physical dysfunction, substantially impacting on quality of life and imposing enormous cost to the healthcare system. Exercise is pivotal to OA management, yet uptake by people with knee OA is inadequate. Limited access to appropriately skilled health professionals, such as physiotherapists, for prescription of an exercise program and support with exercise is a major barrier to optimal care. Internet-enabled video consultations permit widespread reach. However, services offering video consultations with physiotherapists for musculoskeletal conditions are scant in Australia where there is typically no Government or private health insurer funding for such services. The paucity of robust evidence demonstrating video consultations with physiotherapists are clinically effective, safe and cost-effective for knee OA is hampering implementation of, and willingness of healthcare policymakers to pay for, these services.
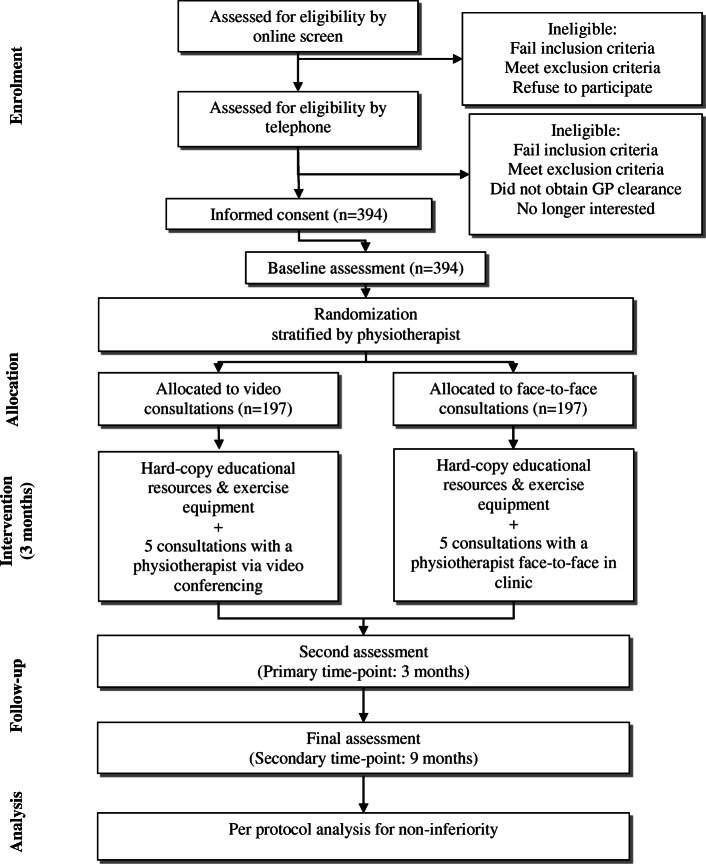
This is an assessor- and participant-blinded, two-arm, pragmatic, comparative effectiveness non-inferiority randomised controlled trial (RCT) conducted in Australia. We are recruiting 394 people from the community with chronic knee pain consistent with a clinical diagnosis of knee OA. Participants are randomly allocated to receive physiotherapy care via i) video-conferencing or; ii) face-to-face consultations. Participants are provided five consultations (30-45 min each) with a physiotherapist over 3 months for prescription of a home-based strengthening exercise program (to be conducted independently at home) and physical activity plan, as well as OA education. Participants in both groups are provided with educational booklets and simple exercise equipment via post. The co-primary outcomes are change in self-reported i) knee pain on walking; and ii) physical function, with a primary end-point of 3 months and a secondary end-point of 9 months. Secondary outcomes include changes in other clinical outcomes (health-related quality of life; therapeutic relationship; global ratings of change; satisfaction with care; self-efficacy; physical activity levels), time and financial costs of attending consultations, healthcare usage and convenience. Non-inferiority will be assessed using the per-protocol dataset.
Findings will determine if video consultations with physiotherapists are non-inferior to traditional face-to-face consultations for management of people with knee OA.
Australian New Zealand Clinical Trials Registry, ACTRN12619001240134. http://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=377672&isReview=true.
膝关节骨关节炎(OA)是一个全球性问题,会导致严重疼痛和身体功能障碍,对生活质量产生重大影响,并给医疗系统带来巨大成本。运动对OA的管理至关重要,但膝关节OA患者的运动参与度不足。获得具备适当技能的医疗专业人员(如物理治疗师)来开具运动计划处方并提供运动支持,是实现最佳护理的主要障碍。基于互联网的视频咨询具有广泛的覆盖范围。然而,在澳大利亚,提供与物理治疗师进行肌肉骨骼疾病视频咨询服务的机构很少,而且通常没有政府或私人健康保险公司为这类服务提供资金。缺乏有力证据证明与物理治疗师进行视频咨询对膝关节OA在临床上有效、安全且具有成本效益,这阻碍了这些服务的实施以及医疗政策制定者为其付费的意愿。
这是一项在澳大利亚进行的评估者和参与者双盲、双臂、实用、比较有效性非劣效性随机对照试验(RCT)。我们正在从社区招募394名患有与膝关节OA临床诊断相符的慢性膝关节疼痛的人。参与者被随机分配接受物理治疗护理,方式为:i)视频会议;或ii)面对面咨询。参与者在3个月内接受5次与物理治疗师的咨询(每次30 - 45分钟),以开具家庭强化运动计划(在家中独立进行)和身体活动计划,以及OA教育。两组参与者均通过邮寄方式获得教育手册和简单的运动设备。共同主要结局是自我报告的:i)行走时膝关节疼痛的变化;ii)身体功能的变化,主要终点为3个月,次要终点为9个月。次要结局包括其他临床结局(与健康相关的生活质量、治疗关系、总体变化评分、护理满意度、自我效能感、身体活动水平)的变化、就诊的时间和财务成本、医疗保健使用情况和便利性。将使用符合方案数据集评估非劣效性。
研究结果将确定与物理治疗师进行视频咨询在管理膝关节OA患者方面是否不劣于传统的面对面咨询。
澳大利亚新西兰临床试验注册中心,ACTRN12619001240134。http://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=377672&isReview=true。