Los Angeles Medical Center, Department of Neurology, Southern California Permanente Medical Group, 1505 N Edgemont, 5thFloor, Los Angeles, CA 90027, USA.
Department of Research & Evaluation, Southern California Permanente Medical Group, 100 S Los Robles Avenue, Pasadena, CA 91101, USA.
Int J Infect Dis. 2020 Oct;99:291-297. doi: 10.1016/j.ijid.2020.07.081. Epub 2020 Aug 6.
To examine outcomes among patients who were treated with the targeted anti-cytokine agents, anakinra or tocilizumab, for COVID-19 -related cytokine storm (COVID19-CS).
We conducted a retrospective cohort study of all SARS-coV2-RNA-positive patients treated with tocilizumab or anakinra in Kaiser Permanente Southern California. Local experts developed and implemented criteria to define COVID19-CS. All variables were extracted from electronic health records.
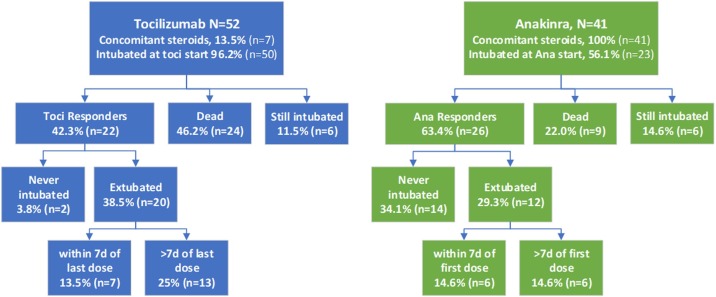
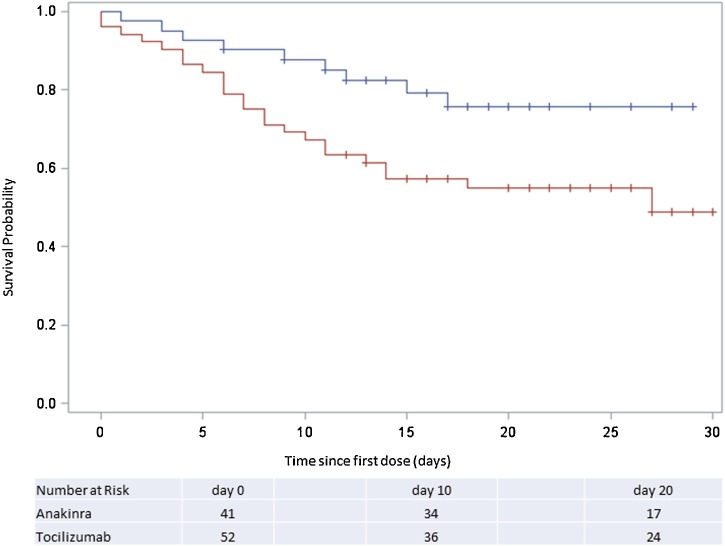
At tocilizumab initiation (n = 52), 50 (96.2%) were intubated, and only seven (13.5%) received concomitant corticosteroids. At anakinra initiation (n = 41), 23 (56.1%) were intubated, and all received concomitant corticosteroids. Fewer anakinra-treated patients died (n = 9, 22%) and more were extubated/never intubated (n = 26, 63.4%) compared to tocilizumab-treated patients (n = 24, 46.2% dead, n = 22, 42.3% extubated/never intubated). Patients who died had more severe sepsis and respiratory failure and met COVID-CS laboratory criteria longer (median = 3 days) compared to those extubated/never intubated (median = 1 day). After accounting for differences in disease severity at treatment initiation, this apparent superiority of anakinra over tocilizumab was no longer statistically significant (propensity score-adjusted hazards ratio 0.46, 95% confidence interval 0.18-1.20).
Prompt identification and treatment of COVID19-CS before intubation may be more important than the specific type of anti-inflammatory treatment. Randomized controlled trials of targeted anti-cytokine treatments and corticosteroids should report the duration of cytokine storm in addition to clinical severity at randomization.
研究接受靶向细胞因子药物(阿那白滞素或托珠单抗)治疗的 COVID-19 相关细胞因子风暴(COVID19-CS)患者的结局。
我们对 Kaiser Permanente Southern California 所有接受托珠单抗或阿那白滞素治疗的 SARS-CoV2-RNA 阳性患者进行了回顾性队列研究。当地专家制定并实施了定义 COVID19-CS 的标准。所有变量均从电子健康记录中提取。
在开始使用托珠单抗时(n = 52),有 50 例(96.2%)患者插管,仅有 7 例(13.5%)接受了皮质类固醇的联合治疗。在开始使用阿那白滞素时(n = 41),有 23 例(56.1%)患者插管,所有患者均接受了皮质类固醇的联合治疗。与接受托珠单抗治疗的患者(n = 24,死亡 46.2%,插管/未插管 42.3%)相比,接受阿那白滞素治疗的患者死亡人数更少(n = 9,22%),且更多患者拔管/未插管(n = 26,63.4%)。死亡患者的严重脓毒症和呼吸衰竭更为严重,符合 COVID-CS 实验室标准的时间更长(中位数 = 3 天),而插管/未插管患者的(中位数 = 1 天)。在考虑到治疗开始时疾病严重程度的差异后,阿那白滞素优于托珠单抗的这种明显优势不再具有统计学意义(倾向评分调整后的危害比 0.46,95%置信区间 0.18-1.20)。
在插管前及时识别和治疗 COVID19-CS 可能比使用特定类型的抗炎治疗更为重要。靶向细胞因子治疗和皮质类固醇的随机对照试验除了报告随机分组时的临床严重程度外,还应报告细胞因子风暴的持续时间。